

Reducing referral delays in colorectal cancer diagnosis: is it about how you ask?
- PMID: 20584706
- PMCID: PMC2965264
- DOI: 10.1136/qshc.2009.033712
Reducing referral delays in colorectal cancer diagnosis: is it about how you ask?
Abstract
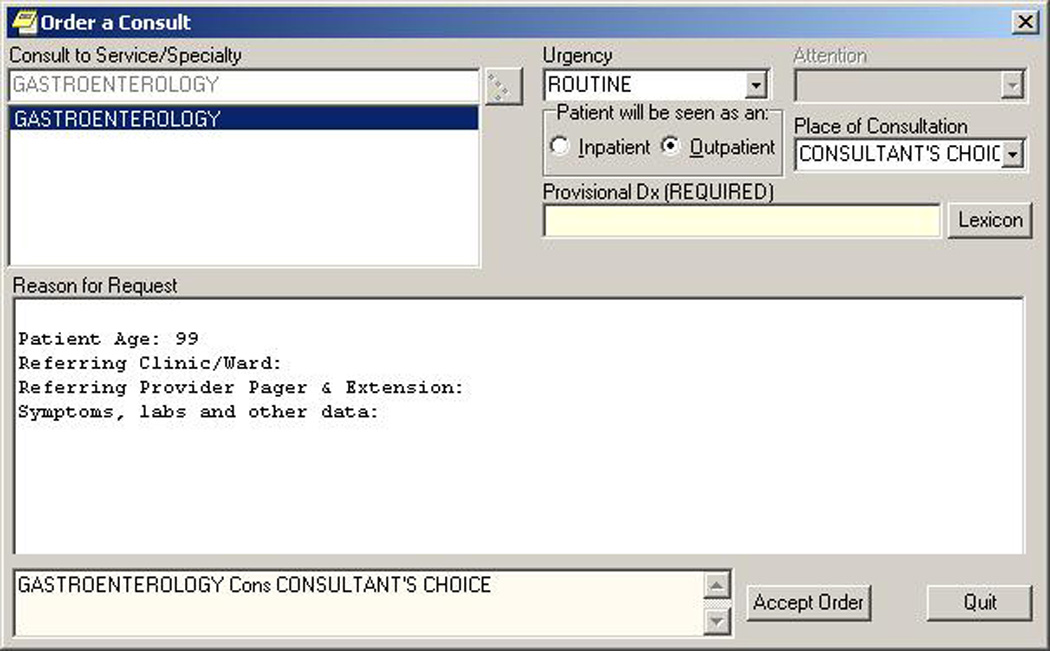
Objectives: Delays in colorectal cancer (CRC) diagnosis related to colonoscopy referrals are not well studied. The authors tested whether certain details of information transmitted through computerised provider order entry (CPOE)-based referrals affected timeliness of diagnostic colonoscopy for patients with newly diagnosed CRC.
Methods: The authors studied a 6-year cohort of all newly diagnosed patients with CRC at a large tertiary care Veterans Affairs hospital and its affiliated multispecialty clinics. Referring providers included primary care clinicians, resident trainees and other specialists. From the colonoscopy referral preceding CRC diagnosis, the authors determined request date, type and frequency of diagnostic clues provided (symptoms, signs, test results), notation of urgency, and documented evidence of verbal contact between referring provider and consultant to expedite referral. The authors compared distributions of proportions of diagnostic clues between patients with a lag of >60 and ≤60 day, and examined predictors of lag time.
Results: Of 367 electronic referrals identified with a median lag of 57 days, 178 (48.5%) had a lag of >60 days. Referrals associated with longer lag times included those with 'positive faecal occult blood test' (92 days, p<0.0001), 'haematochesia' (75 days, p=0.02), 'history of polyps' (221 days, p=0.0006) and when 'screening' (vs specific symptoms) was given as the reason for diagnostic colonoscopy (203 days, p=0.002). Independent predictors of shorter wait times included three diagnostic clues, notation of urgency and documentation of verbal contact.
Conclusions: Attention to certain details of diagnostic information provided to consultants through CPOE-based referrals may help reduce delays in CRC diagnosis.
Conflict of interest statement
None
Figures
Similar articles
-
Postreferral colonoscopy delays in diagnosis of colorectal cancer: a mixed-methods analysis.Qual Manag Health Care. 2012 Oct-Dec;21(4):252-61. doi: 10.1097/QMH.0b013e31826d1f28. Qual Manag Health Care. 2012. PMID: 23011072 Free PMC article.
-
Wait times from presentation to treatment for colorectal cancer: a population-based study.Can J Gastroenterol. 2010 Jan;24(1):33-9. doi: 10.1155/2010/692151. Can J Gastroenterol. 2010. PMID: 20186354 Free PMC article.
-
Straight-to-test colonoscopy for 2-week-wait referrals improves time to diagnosis of colorectal cancer and is feasible in a high-volume unit.Colorectal Dis. 2017 Sep;19(9):819-826. doi: 10.1111/codi.13667. Colorectal Dis. 2017. PMID: 28342189
-
Electronic Trigger-Based Intervention to Reduce Delays in Diagnostic Evaluation for Cancer: A Cluster Randomized Controlled Trial.J Clin Oncol. 2015 Nov 1;33(31):3560-7. doi: 10.1200/JCO.2015.61.1301. Epub 2015 Aug 24. J Clin Oncol. 2015. PMID: 26304875 Free PMC article. Clinical Trial.
-
Factors contributing to time to diagnosis in symptomatic colorectal cancer: A scoping review.Eur J Cancer Care (Engl). 2021 May;30(3):e13397. doi: 10.1111/ecc.13397. Epub 2020 Dec 30. Eur J Cancer Care (Engl). 2021. PMID: 33377574
Cited by
-
The 2012 SAGE wait times program: Survey of Access to GastroEnterology in Canada.Can J Gastroenterol. 2013 Feb;27(2):83-9. doi: 10.1155/2013/143018. Can J Gastroenterol. 2013. PMID: 23472243 Free PMC article.
-
Patient-Reported Attributions for Missed Colonoscopy Appointments in Two Large Healthcare Systems.Dig Dis Sci. 2016 Jul;61(7):1853-61. doi: 10.1007/s10620-016-4096-3. Epub 2016 Mar 12. Dig Dis Sci. 2016. PMID: 26971093
-
Bringing an organizational perspective to the optimal number of colorectal cancer screening options debate.J Gen Intern Med. 2012 Mar;27(3):376-80. doi: 10.1007/s11606-011-1870-y. Epub 2011 Sep 14. J Gen Intern Med. 2012. PMID: 21915765 Free PMC article. Review.
-
Disruptive Innovation: Implementation of Electronic Consultations in a Veterans Affairs Health Care System.JMIR Med Inform. 2016 Feb 12;4(1):e6. doi: 10.2196/medinform.4801. JMIR Med Inform. 2016. PMID: 26872820 Free PMC article.
-
Postreferral colonoscopy delays in diagnosis of colorectal cancer: a mixed-methods analysis.Qual Manag Health Care. 2012 Oct-Dec;21(4):252-61. doi: 10.1097/QMH.0b013e31826d1f28. Qual Manag Health Care. 2012. PMID: 23011072 Free PMC article.
References
-
- Gandhi TK, Kachalia A, Thomas EJ, et al. Missed and delayed diagnoses in the ambulatory setting: A study of closed malpractice claims. Ann Intern Med. 2006;145:488–496. - PubMed
-
- Fisher DA, Jeffreys A, Coffman CJ, Fasanella K. Barriers to full colon evaluation for a positive fecal occult blood test. Cancer Epidemiol Biomarkers Prev. 2006;15:1232–1235. - PubMed
-
- Yabroff K, Washington KS, Leader A, Neilson E, Mandelblatt J. Is the Promise of Cancer-Screening Programs Being Compromised? Quality of Follow-Up Care after Abnormal Screening Results. Med Care Res Rev. 2003;60:294–331. - PubMed
-
- Freeman HP, Muth BJ, Kerner JF. Expanding access to cancer screening and clinical follow-up among the medically underserved. Cancer Pract. 1995;3:19–30. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical