

Diagnostic pitfalls in newborns and babies with blisters and erosions
- PMID: 20585476
- PMCID: PMC2879860
- DOI: 10.1155/2009/320403
Diagnostic pitfalls in newborns and babies with blisters and erosions
Abstract
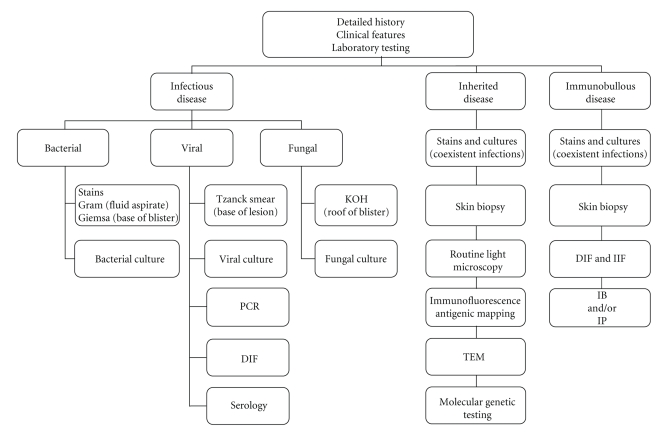
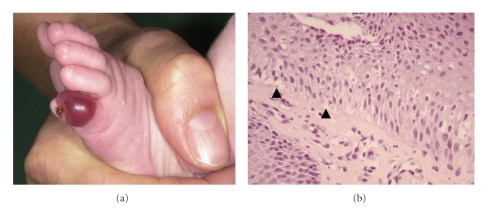
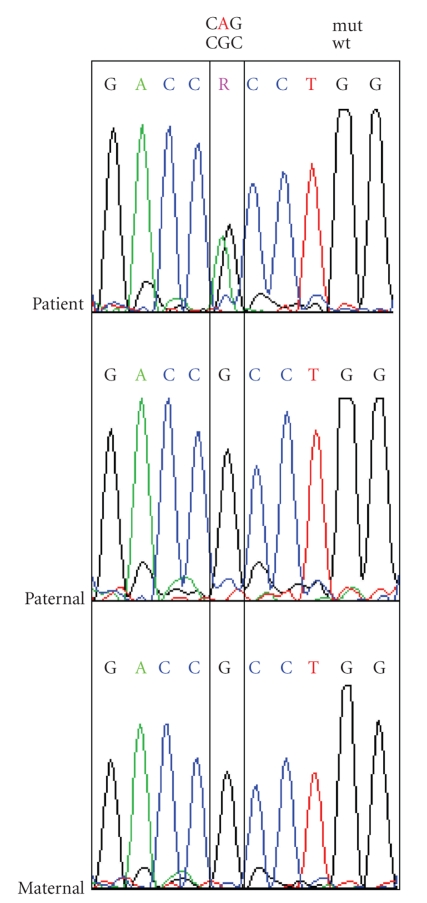
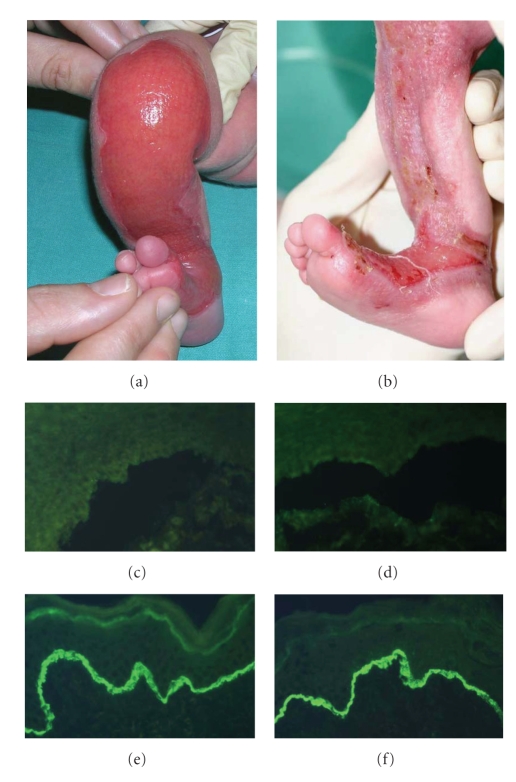
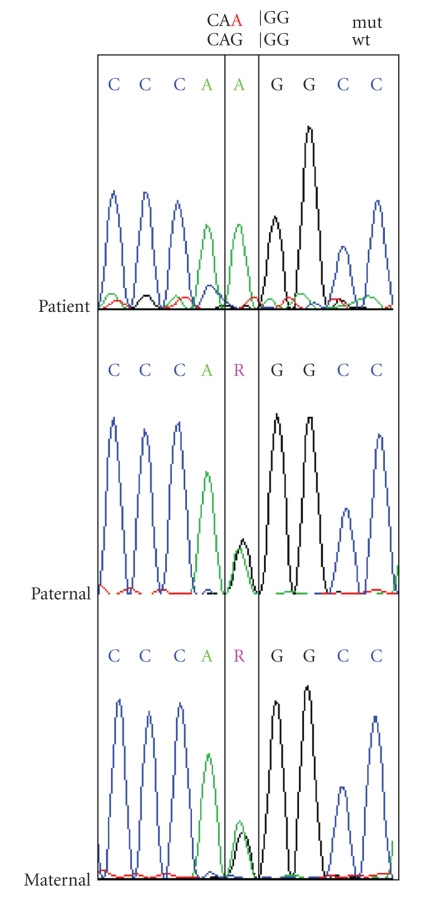
Establishing the correct diagnosis in newborns presenting with blisters and erosions is not always a straightforward process. Many different disease entities including acquired (i.e., infectious, immunobullous, traumatic) and inherited disorders have to be taken into consideration. Similarities in clinical appearance, colonization and/or superinfections of preexisting skin lesions, as well as the absence of late changes in the neonate often pose significant diagnostic challenges. In this paper we discuss by giving examples the process of making an accurate diagnosis of blistering skin diseases in the neonatal period on the basis of a diagnostic algorithm. In addition, we provide an overview of the rational use and the limitations of laboratory procedures such as microbial testing, routine light microscopy, immunofluorescence antigen mapping, transmission electron microscopy, and molecular genetic analysis.
Figures


Similar articles
-
Orf-induced immunobullous disease: A distinct autoimmune blistering disorder.J Am Acad Dermatol. 2008 Jan;58(1):49-55. doi: 10.1016/j.jaad.2007.08.029. Epub 2007 Oct 4. J Am Acad Dermatol. 2008. PMID: 17919774
-
How to Deal with Skin Biopsy in an Infant with Blisters?Dermatopathology (Basel). 2021 Jun 4;8(2):159-175. doi: 10.3390/dermatopathology8020022. Dermatopathology (Basel). 2021. PMID: 34199848 Free PMC article. Review.
-
Bullous Pemphigoid Masquerading as Erythema Annulare Centrifugum.Acta Dermatovenerol Croat. 2017 Oct;25(3):255-256. Acta Dermatovenerol Croat. 2017. PMID: 29252183
-
Inherited epidermolysis bullosa: new diagnostic criteria and classification.Clin Dermatol. 2012 Jan-Feb;30(1):70-7. doi: 10.1016/j.clindermatol.2011.03.012. Clin Dermatol. 2012. PMID: 22137229 Review.
-
End of the century overview of skin blisters.Arch Dermatol. 2000 Jan;136(1):106-12. doi: 10.1001/archderm.136.1.106. Arch Dermatol. 2000. PMID: 10632212 Review.
Cited by
-
Maternal-Fetal Perinatal Transmission of Staphylococcal Infections: A Report of Two Neonates.Case Rep Pediatr. 2020 Jun 16;2020:8886049. doi: 10.1155/2020/8886049. eCollection 2020. Case Rep Pediatr. 2020. PMID: 32607269 Free PMC article.
-
A Sporadic Neonatal Case of Epidermolysis Bullosa Simplex Generalized Intermediate with KRT5 and KRT14 Gene Mutations.AJP Rep. 2016 Mar;6(1):e108-11. doi: 10.1055/s-0035-1570386. AJP Rep. 2016. PMID: 26929861 Free PMC article.
-
Staphylococcal Infections and Neonatal Skin: Data from Literature and Suggestions for the Clinical Management from Four Challenging Patients.Antibiotics (Basel). 2023 Mar 23;12(4):632. doi: 10.3390/antibiotics12040632. Antibiotics (Basel). 2023. PMID: 37106994 Free PMC article. Review.
References
-
- Shwayder T, Akland T. Neonatal skin barrier: structure, function, and disorders. Dermatologic Therapy. 2005;18(2):87–103. - PubMed
-
- Eady RAJ. Epidermolysis bullosa. In: Champion RH, Burton JL, Burns DA, Breathnach SM, editors. Textbook of Dermatology. 6th edition. Oxford, UK: Blackwell; 1998. pp. 1817–1844.
-
- Schuilenga-Hut PH, Vlies P, Jonkman MF, Waanders E, Buys CH, Scheffer H. Mutation analysis of the entire keratin 5 and 14 genes in patients with epidermolysis bullosa simplex and identification of novel mutations. Human Mutation. 2003;21(4):p. 447. - PubMed
-
- Coulombe PA, Hutton ME, Letai A, Hebert A, Paller AS, Fuchs E. Point mutations in human keratin 14 genes of epidermolysis bullosa simplex patients: genetic and functional analyses. Cell. 1991;66(6):1301–1311. - PubMed
-
- Stephens K, Sybert VP, Wijsman EM, Ehrlich P, Spencer A. A keratin 14 mutational hot spot for epidermolysis bullosa simplex, Dowling-Meara: implications for diagnosis. Journal of Investigative Dermatology. 1993;101(2):240–243. - PubMed
LinkOut - more resources
Full Text Sources
