

Depression, antidepressant use and mortality in later life: the Health In Men Study
- PMID: 20585644
- PMCID: PMC2890408
- DOI: 10.1371/journal.pone.0011266
Depression, antidepressant use and mortality in later life: the Health In Men Study
Abstract
Context: Depression is associated with increased mortality, but it is unclear if this relationship is dose-dependent and if it can be modified by treatment with antidepressants.
Objective: To determine if (1) the association between depression and mortality is independent of other common potential causes of death in later life, (2) there is a dose-response relationship between increasing severity of depression and mortality rates, and (3) the use of antidepressant drugs reduces mortality rates.
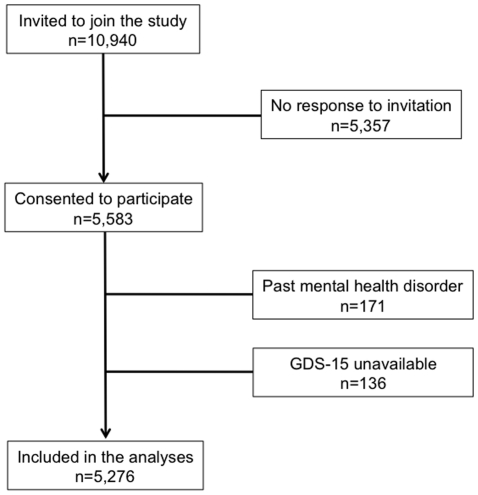
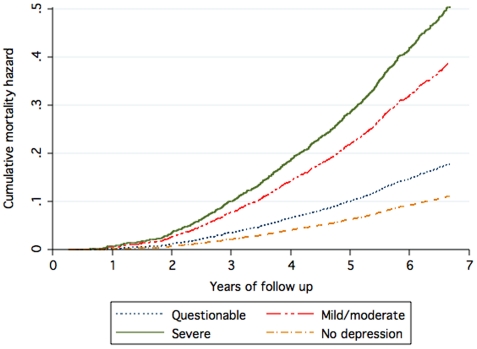
Methods: Cohort study of 5,276 community-dwelling men aged 68-88 years living in Perth, Australia. We used the Geriatric Depression Scale 15-items (GDS-15) to ascertain the presence and severity of depression. GDS-15 > or = 7 indicates the presence of clinically significant depression. Men were also grouped according to the severity of symptoms: "no symptoms" (GDS-15 = 0), "questionable" (1 < or = GDS-15 < or = 4), "mild to moderate" (5 < or = GDS-15 < or = 9), and "severe" (GDS-15 > or = 10). Participants listed all medications used regularly. We used the Western Australian Data Linkage System to monitor mortality.
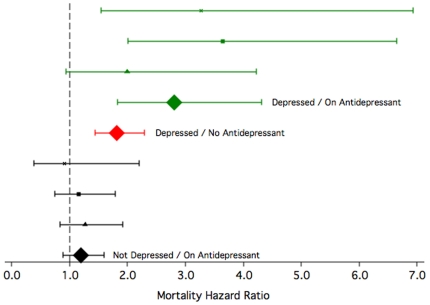
Results: There were 883 deaths between the study assessment and the 30th June 2008 (mean follow-up of participants: 6.0+/-1.1 years). The adjusted mortality hazard (MH) of men with clinically significant depression was 1.98 (95%CI = 1.61-2.43), and increased with the severity of symptoms: 1.39 (95%CI = 1.13-1.71) for questionable, 2.71 (95%CI = 2.13-3.46) for mild/moderate, and 3.32 (95%CI: 2.31-4.78) for severe depression. The use of antidepressants increased MH (HR = 1.31, 95%CI = 1.02-1.68). Compared with men who were not depressed and were not taking antidepressants, MH increased from 1.22 (95%CI = 0.91-1.63) for men with no depression who were using antidepressants to 1.85 (95%CI = 1.47-2.32) for participants who were depressed but were not using antidepressants, and 2.97 (95%CI = 1.94-4.54) for those who were depressed and were using antidepressants. All analyses were adjusted for age, educational attainment, migrant status, physical activity, smoking and alcohol use and the Charlson comorbidity index.
Conclusions: The mortality associated with depression increases with the severity of depressive symptoms and is largely independent of comorbid conditions. The use of antidepressants does not reduce the mortality rates of older men with persistent symptoms of depression.
Conflict of interest statement
Figures
Similar articles
-
Depression, antidepressants and the risk of cardiovascular events and death in older men.Maturitas. 2019 Oct;128:4-9. doi: 10.1016/j.maturitas.2019.06.009. Epub 2019 Jun 28. Maturitas. 2019. PMID: 31561821
-
Association of detected depression and undetected depressive symptoms with long-term mortality in a cohort of institutionalised older people.Epidemiol Psychiatr Sci. 2017 Apr;26(2):189-198. doi: 10.1017/S2045796015001171. Epub 2016 Jan 12. Epidemiol Psychiatr Sci. 2017. PMID: 26753838 Free PMC article.
-
Late-life depression and mortality: influence of gender and antidepressant use.Br J Psychiatry. 2008 Jan;192(1):12-8. doi: 10.1192/bjp.bp.107.039164. Br J Psychiatry. 2008. PMID: 18174502
-
Cardiovascular diseases do not influence the mental health outcome of older men with depression over 6 years.J Affect Disord. 2013 Jan 25;144(3):248-52. doi: 10.1016/j.jad.2012.06.043. Epub 2012 Jul 31. J Affect Disord. 2013. PMID: 22858261
-
Adjuvant therapy with antidepressants for the management of inflammatory bowel disease.Cochrane Database Syst Rev. 2019 Apr 12;4(4):CD012680. doi: 10.1002/14651858.CD012680.pub2. Cochrane Database Syst Rev. 2019. PMID: 30977111 Free PMC article.
Cited by
-
The increasing burden of depression.Neuropsychiatr Dis Treat. 2011;7(Suppl 1):3-7. doi: 10.2147/NDT.S19617. Epub 2011 May 31. Neuropsychiatr Dis Treat. 2011. PMID: 21750622 Free PMC article.
-
Depressive Symptoms in the Elderly-An Early Symptom of Dementia? A Systematic Review.Front Pharmacol. 2020 Feb 7;11:34. doi: 10.3389/fphar.2020.00034. eCollection 2020. Front Pharmacol. 2020. PMID: 32116710 Free PMC article.
-
Primum non nocere: an evolutionary analysis of whether antidepressants do more harm than good.Front Psychol. 2012 Apr 24;3:117. doi: 10.3389/fpsyg.2012.00117. eCollection 2012. Front Psychol. 2012. PMID: 22536191 Free PMC article.
-
Pain severity predicts depressive symptoms over and above individual illnesses and multimorbidity in older adults.BMC Psychiatry. 2017 May 4;17(1):166. doi: 10.1186/s12888-017-1334-y. BMC Psychiatry. 2017. PMID: 28472936 Free PMC article.
-
Chronic Systemic Inflammation Is Associated With Symptoms of Late-Life Depression: The ARIC Study.Am J Geriatr Psychiatry. 2020 Jan;28(1):87-98. doi: 10.1016/j.jagp.2019.05.011. Epub 2019 May 21. Am J Geriatr Psychiatry. 2020. PMID: 31182350 Free PMC article.
References
-
- Prince M, Patel V, Saxena S, Maj M, Maselko J, et al. No health without mental health. Lancet. 2007;370:859–877. - PubMed
-
- Kessler RC, Berglund P, Demler O, Jin R, Koretz D, et al. The epidemiology of major depressive disorder: results from the National Comorbidity Survey Replication (NCS-R). JAMA. 2003;289:3095–3105. - PubMed
-
- Tiemeier H, Breteler MM, Hofman A, Stijnen T. A multivariate score objectively assessed health of depressed elderly. J Clin Epidemiol. 2005;58:1134–1141. - PubMed
-
- Surtees PG, Wainwright NW, Luben RN, Wareham NJ, Bingham SA, et al. Depression and ischemic heart disease mortality: evidence from the EPIC-Norfolk United Kingdom prospective cohort study. Am J Psychiatry. 2008;165:515–523. - PubMed
-
- Ensinck KT, Schuurman AG, van den Akker M, Metsemakers JF, Kester AD, et al. Is there an increased risk of dying after depression? Am J Epidemiol. 2002;156:1043–1048. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
