

Injury hospitalization as a marker for emergency medical services use in elderly patients
- PMID: 20586586
- PMCID: PMC2992380
- DOI: 10.3109/10903127.2010.493986
Injury hospitalization as a marker for emergency medical services use in elderly patients
Abstract
Background: The elderly utilize emergency medical services (EMS) at a higher rate than younger patients, yet little is known about the influence of injury on subsequent EMS utilization and costs.
Objective: To assess injury hospitalization as a potential marker for subsequent EMS utilization and costs by Medicare patients.
Methods: This observational study analyzed a retrospective cohort of all Medicare patients (> or = 67 years old) with an International Classification of Diseases, Ninth Revision (ICD-9) injury diagnosis admitted to 125 Oregon and Washington hospitals during 2001 and 2002 who survived to hospital discharge. The numbers of EMS transports and the total EMS costs were compared one year before and one year following the index hospitalization.
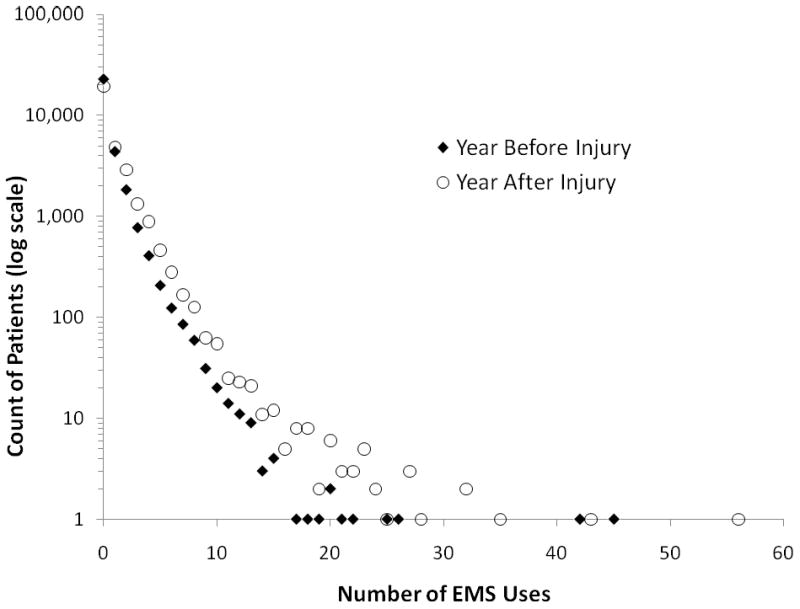
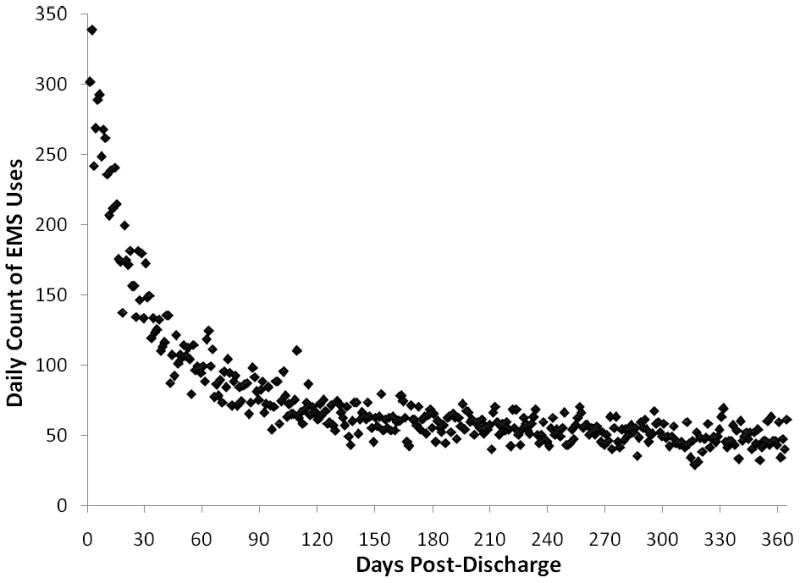
Results: There were 30,655 injured elders in our cohort. Their median ICD-9-based injury severity score was 0.97, with 4.1% meeting a definition of serious injury and 37% having hip fractures. The mean (range) numbers of EMS transports before and after the injury were 0.5 (0-45) and 0.9 (0-56), for an unadjusted incidence rate ratio (IRR) of 1.7 (95% confidence interval [CI] 1.7-1.8). The increase in EMS utilization following an injury hospitalization was even greater after adjusting for risk period and other model predictors (IRR 2.4, 95% CI 2.3-2.5). Annual mean EMS costs rose 74% following the injury hospitalization, from $211 to $367 per person. The greatest increase was in nonemergent EMS use, accounting for 67% of the increase in the number of uses. Institutionalization in a skilled nursing or rehabilitation facility either before or after injury was strongly associated with the need for EMS care.
Conclusion: An injury hospitalization in the elderly serves as a sentinel marker for an abrupt increase in EMS utilization and costs, even after accounting for confounders.
Figures
Similar articles
-
Evaluation of Rural vs Urban Trauma Patients Served by 9-1-1 Emergency Medical Services.JAMA Surg. 2017 Jan 1;152(1):11-18. doi: 10.1001/jamasurg.2016.3329. JAMA Surg. 2017. PMID: 27732713 Free PMC article.
-
The epidemiology of elderly falls attended by emergency medical services in Victoria, Australia.Injury. 2018 Sep;49(9):1712-1719. doi: 10.1016/j.injury.2018.06.038. Epub 2018 Jun 25. Injury. 2018. PMID: 30126534
-
Is futile care in the injured elderly an important target for cost savings?J Trauma Acute Care Surg. 2012 Jul;73(1):146-51. doi: 10.1097/TA.0b013e318251f9aa. J Trauma Acute Care Surg. 2012. PMID: 22743384 Free PMC article.
-
Comparison of Injured Older Adults Included in vs Excluded From Trauma Registries With 1-Year Follow-up.JAMA Surg. 2019 Sep 1;154(9):e192279. doi: 10.1001/jamasurg.2019.2279. Epub 2019 Sep 18. JAMA Surg. 2019. PMID: 31290955 Free PMC article.
-
A Comparison of Scoring Systems for Predicting Short- and Long-term Survival After Trauma in Older Adults.Acad Emerg Med. 2019 Jun;26(6):621-630. doi: 10.1111/acem.13727. Epub 2019 Apr 3. Acad Emerg Med. 2019. PMID: 30884022
Cited by
-
Functional Decline Predicts Emergency Department Use in Veterans With Dementia.Am J Alzheimers Dis Other Demen. 2014 Jun;29(4):362-71. doi: 10.1177/1533317513518655. Epub 2014 Jan 9. Am J Alzheimers Dis Other Demen. 2014. PMID: 24413540 Free PMC article.
References
-
- Wofford JL, Moran WP, Heuser MD, Schwartz E, Velez R, Mittelmark MB. Emergency Medical Transport of the Elderly: A Population-Based Study. American Journal of Emergency Medicine. 1995;13(3):297–300. - PubMed
-
- McConnel CE, Wilson RW. The Demand for Prehospital Emergency Services in an Aging Society. Social Science Medicine. 1998;46(8):1027–31. - PubMed
-
- Spaite DW, Criss EA, Valenzuela TD, Meislin HW, Ross J. Geriatric Injury: An Analysis of Prehospital Demographics, Mechanisms, and Patterns. Annals of Emergency Medicine. 1990;19(12):1418–1421. - PubMed
-
- Pitts SR, Niska RW, Xu J, Burt CW. National Hospital Ambulatory Medical Care Survey: 2006 Emergency Department Summary. [April 19, 2009]. Available at: http://www.cdc.gov/nchs/data/nhsr/nhsr007.pdf. - PubMed
-
- Dickinson ET, Verdile VP, Kostyun CT, Salluzzo RF. Geriatric Use of Emergency Medical Services. Annals of Emergency Medicine. 1996 February;27(2):199–203. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical