

Low retention of HIV-infected patients on antiretroviral therapy in 11 clinical centres in West Africa
- PMID: 20586958
- PMCID: PMC2919326
- DOI: 10.1111/j.1365-3156.2010.02505.x
Low retention of HIV-infected patients on antiretroviral therapy in 11 clinical centres in West Africa
Abstract
Objective: To study factors associated with the probability of retention in antiretroviral therapy (ART) programmes in West Africa.
Methods: The International epidemiologic Databases to Evaluate AIDS (IeDEA) in West Africa is a prospective, operational, observational cohort study based on collaboration between 11 cohorts of HIV-infected adult patients in Benin, Côte d'Ivoire, Gambia, Mali and Senegal. All patients aged 16 and older at ART initiation, with documented gender and date of ART initiation, were included. For those with at least 1 day of follow-up, Kaplan-Meier method and Weibull regression model were used to estimate the 12-month probability of retention in care and the associated factors.
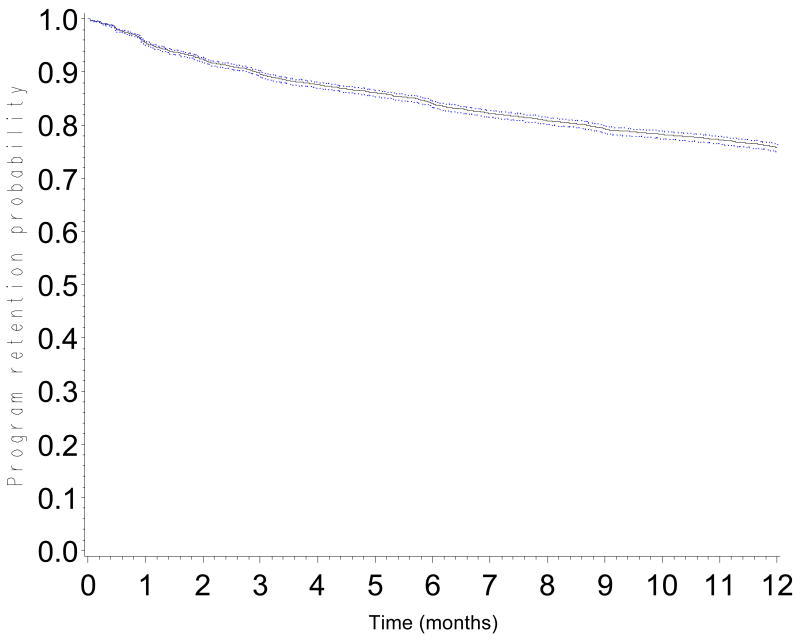
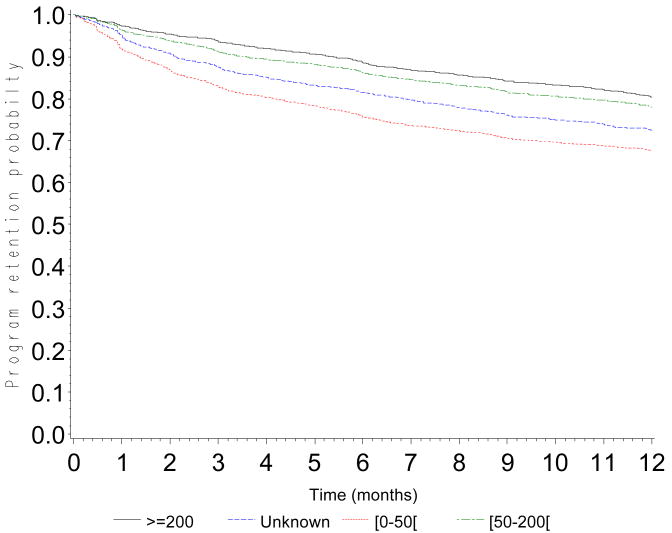
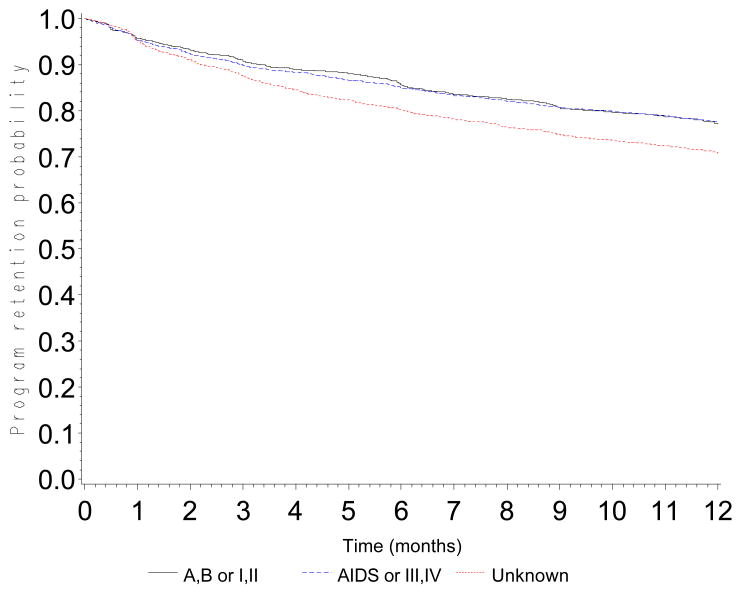
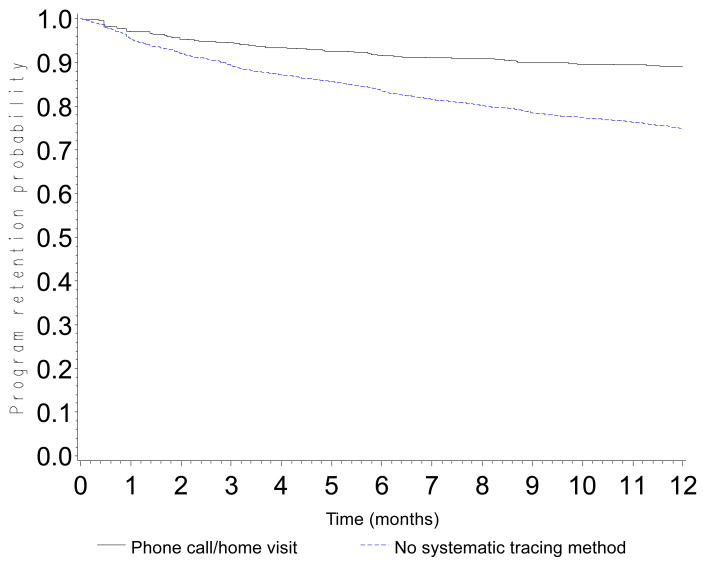
Results: In this data merger, 14 352 patients (61% female) on ART were included. Median age was 37 (interquartile range (IQR): 31-44 years) and median CD4 count at baseline was 131 cells/mm(3) (IQR: 48-221 cells/mm(3)). The first-line regimen was NNRTI-based for 78% of patients, protease inhibitor-based for 17%, and three NRTIs for 3%. The probability of retention was 0.90 [95% confidence interval (CI): 0.89-0.90] at 3 months, 0.84 (95% CI: 0.83-0.85) at 6 months and 0.76 (95% CI: 0.75-0.77) at 12 months. The probability of retention in care was lower in patients with baseline CD4 count <50 cells/mm(3) [adjusted hazard ratio (aHR) = 1.37; 95% CI: 1.27-1.49; P < 0.0001] (reference CD4 > 200 cells/mm(3), in men (aHR = 1.17; 95% CI: 1.10-1.24; P = 0.0002), in younger patients (<30 years) (aHR = 1.10; 95% CI: 1.03-1.19; P = 0.01) and in patients with low haemoglobinaemia <8 g/dl (aHR = 1.33; 95% CI: 1.21-1.45; P < 0.0001). Availability of funds for systematic tracing was associated with better retention (aHR = 0.29; 95% CI: 0.16-0.55; P = 0.001).
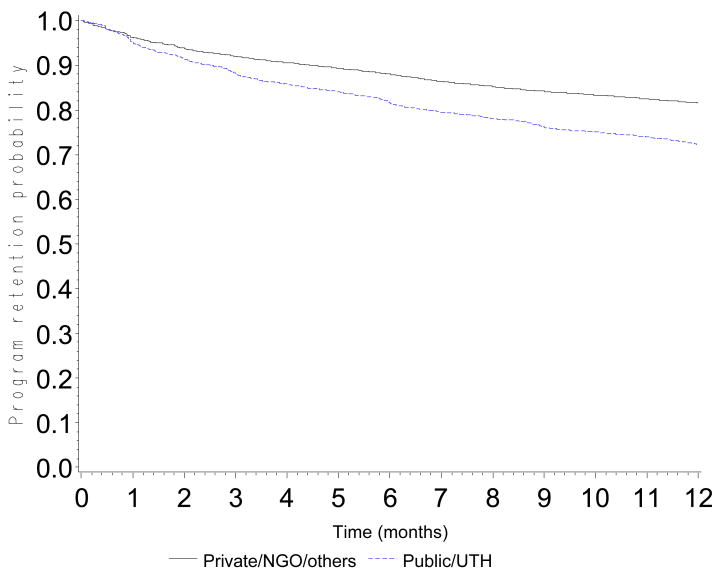
Conclusions: Close follow-up, promoting early access to care and ART and a decentralized system of care may improve the retention in care of HIV-infected patients on ART.
Figures
References
-
- Anglaret X, Toure S, Gourvellec G, et al. Impact of vital status investigation procedures on estimates of survival in cohorts of HIV-infected patients from Sub-Saharan Africa. Journal of Acquired Immune Deficiency Syndrome. 2004;35:320–3. - PubMed
-
- Braitstein P, Brinkhof MW, Dabis F, et al. Mortality of HIV-1-infected patients in the first year of antiretroviral therapy: comparison between low-income and high-income countries. Lancet. 2006;367:817–24. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
