

Verbal autopsy interpretation: a comparative analysis of the InterVA model versus physician review in determining causes of death in the Nairobi DSS
- PMID: 20587026
- PMCID: PMC2902422
- DOI: 10.1186/1478-7954-8-21
Verbal autopsy interpretation: a comparative analysis of the InterVA model versus physician review in determining causes of death in the Nairobi DSS
Abstract
Background: Developing countries generally lack complete vital registration systems that can produce cause of death information for health planning in their populations. As an alternative, verbal autopsy (VA) - the process of interviewing family members or caregivers on the circumstances leading to death - is often used by Demographic Surveillance Systems to generate cause of death data. Physician review (PR) is the most common method of interpreting VA, but this method is a time- and resource-intensive process and is liable to produce inconsistent results. The aim of this paper is to explore how a computer-based probabilistic model, InterVA, performs in comparison with PR in interpreting VA data in the Nairobi Urban Health and Demographic Surveillance System (NUHDSS).
Methods: Between August 2002 and December 2008, a total of 1,823 VA interviews were reviewed by physicians in the NUHDSS. Data on these interviews were entered into the InterVA model for interpretation. Cause-specific mortality fractions were then derived from the cause of death data generated by the physicians and by the model. We then estimated the level of agreement between both methods using Kappa statistics.
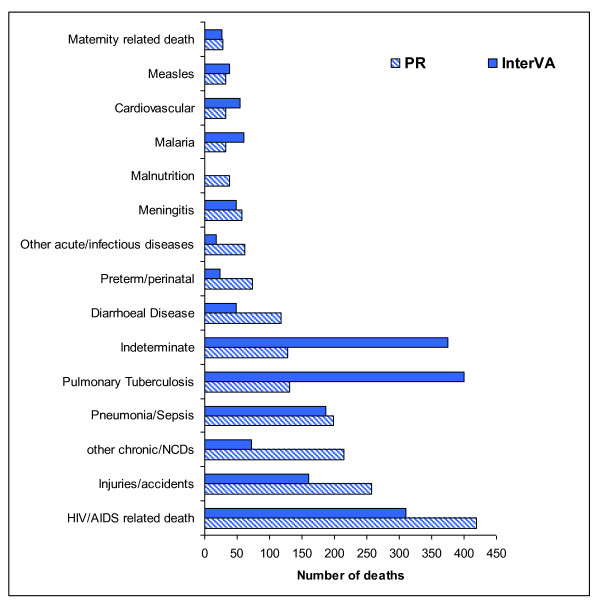
Results: The level of agreement between individual causes of death assigned by both methods was only 35% (kappa = 0.27, 95% CI: 0.25 - 0.30). However, the patterns of mortality as determined by both methods showed a high burden of infectious diseases, including HIV/AIDS, tuberculosis, and pneumonia, in the study population. These mortality patterns are consistent with existing knowledge on the burden of disease in underdeveloped communities in Africa.
Conclusions: The InterVA model showed promising results as a community-level tool for generating cause of death data from VAs. We recommend further refinement to the model, its adaptation to suit local contexts, and its continued validation with more extensive data from different settings.
Figures
Similar articles
-
Causes and circumstances of maternal death: a secondary analysis of the Community-Level Interventions for Pre-eclampsia (CLIP) trials cohort.Lancet Glob Health. 2021 Sep;9(9):e1242-e1251. doi: 10.1016/S2214-109X(21)00263-1. Epub 2021 Jul 29. Lancet Glob Health. 2021. PMID: 34332699 Free PMC article. Clinical Trial.
-
Validating physician-certified verbal autopsy and probabilistic modeling (InterVA) approaches to verbal autopsy interpretation using hospital causes of adult deaths.Popul Health Metr. 2011 Aug 5;9:49. doi: 10.1186/1478-7954-9-49. Popul Health Metr. 2011. PMID: 21819603 Free PMC article.
-
Validating the InterVA model to estimate the burden of mortality from verbal autopsy data: a population-based cross-sectional study.PLoS One. 2013 Sep 13;8(9):e73463. doi: 10.1371/journal.pone.0073463. eCollection 2013. PLoS One. 2013. PMID: 24058474 Free PMC article.
-
Estimating causes of death where there is no medical certification: evolution and state of the art of verbal autopsy.Glob Health Action. 2021 Oct 26;14(sup1):1982486. doi: 10.1080/16549716.2021.1982486. Glob Health Action. 2021. PMID: 35377290 Free PMC article. Review.
-
Validation of verbal autopsy methods for assessment of child mortality in sub-Saharan Africa and the policy implication: a rapid review.Pan Afr Med J. 2019 Aug 22;33:318. doi: 10.11604/pamj.2019.33.318.16405. eCollection 2019. Pan Afr Med J. 2019. PMID: 31692720 Free PMC article. Review.
Cited by
-
Comparative performance of verbal autopsy methods in identifying causes of adult mortality: A case study in India.Indian J Med Res. 2021 Apr;154(4):631-640. doi: 10.4103/ijmr.IJMR_14_19. Indian J Med Res. 2021. PMID: 35435349 Free PMC article.
-
Pattern of all-causes and cause-specific mortality in an area with progressively declining malaria burden in Korogwe district, north-eastern Tanzania.Malar J. 2018 Feb 27;17(1):97. doi: 10.1186/s12936-018-2240-6. Malar J. 2018. PMID: 29482553 Free PMC article.
-
An improved method for physician-certified verbal autopsy reduces the rate of discrepancy: experiences in the Nouna Health and Demographic Surveillance Site (NHDSS), Burkina Faso.Popul Health Metr. 2011 Aug 4;9:34. doi: 10.1186/1478-7954-9-34. Popul Health Metr. 2011. PMID: 21816102 Free PMC article.
-
Methodological challenges in measuring vaccine effectiveness using population cohorts in low resource settings.Vaccine. 2015 Sep 11;33(38):4748-55. doi: 10.1016/j.vaccine.2015.07.062. Epub 2015 Jul 30. Vaccine. 2015. PMID: 26235370 Free PMC article. Review.
-
Evaluating the performance of interpreting Verbal Autopsy 3.2 model for establishing pulmonary tuberculosis as a cause of death in Ethiopia: a population-based cross-sectional study.BMC Public Health. 2012 Nov 29;12:1039. doi: 10.1186/1471-2458-12-1039. BMC Public Health. 2012. PMID: 23190770 Free PMC article.
References
LinkOut - more resources
Full Text Sources
Research Materials
