

Ventricular-arterial uncoupling in heart failure with preserved ejection fraction after myocardial infarction in dogs - invasive versus echocardiographic evaluation
- PMID: 20587034
- PMCID: PMC2902405
- DOI: 10.1186/1471-2261-10-32
Ventricular-arterial uncoupling in heart failure with preserved ejection fraction after myocardial infarction in dogs - invasive versus echocardiographic evaluation
Abstract
Background: Heart failure with preserved left ventricular ejection fraction and abnormal diastolic function is commonly observed after recovery from an acute myocardial infarction. The aim of this study was to investigate the physiopathology of heart failure with preserved ejection fraction in a model of healed myocardial infarction in dogs.
Methods: Echocardiography, levels of neurohormones and conductance catheter measurements of left ventricular pressure-volume relationships were obtained in 17 beagle dogs 2 months after a coronary artery ligation, and in 6 controls.
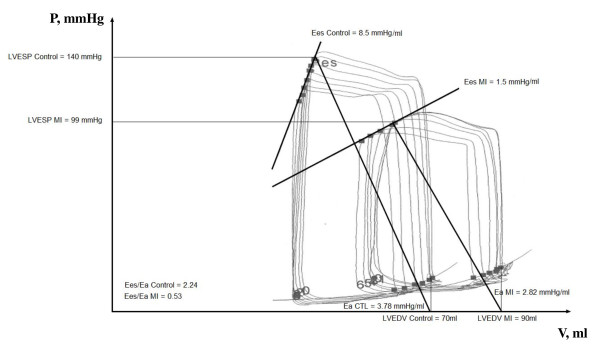
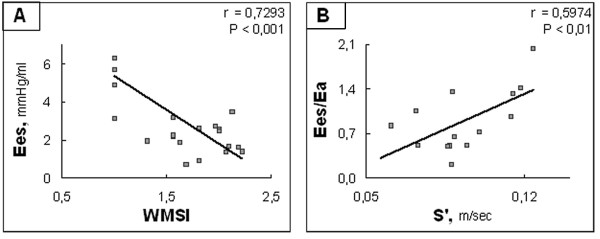
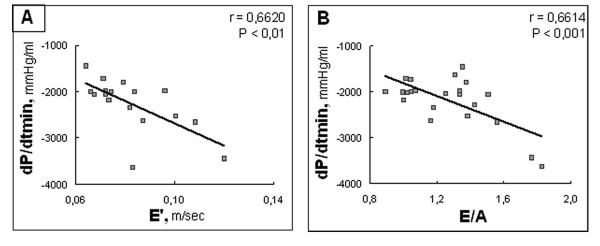
Results: Healed myocardial infarction was associated with preserved echocardiographic left ventricular ejection fraction (0.57 +/- 0.01, mean +/- SEM) and altered Doppler mitral indices of diastolic function. NT-proBNP was increased, aldosterone was decreased, and norepinephrine was unchanged. Invasive measurements showed a markedly decreased end-systolic elastance (2.1 +/- 0.2 vs 6.1 +/- 0.8, mmHg/ml, p < 0.001) and end-systolic elastance to effective arterial elastance ratio (0.6 +/- 0.1 vs 1.4 +/- 0.2, p < 0.001), with altered active relaxation (dP/dtmin -1992 +/- 71 vs -2821 +/- 305, mmHg/s, p < 0.01) but preserved left ventricular capacitance (70 +/- 6 vs 61 +/- 3, ml at 20 mmHg, p = NS) and stiffness constant. Among echocardiographic variables, the wall motion score index was the most reliable indicator of cardiac contractility while E', E/A and E'/A' were correlated to dP/dtmin.
Conclusions: In the canine model of healed myocardial infarction induced by coronary ligation, heart failure is essentially characterized by an altered contractility with left ventricular-arterial uncoupling despite vascular compensation rather than by abnormal diastolic function.
Figures
Similar articles
-
Functional iron deficiency and diastolic function in heart failure with preserved ejection fraction.Int J Cardiol. 2013 Oct 12;168(5):4652-7. doi: 10.1016/j.ijcard.2013.07.185. Epub 2013 Jul 30. Int J Cardiol. 2013. PMID: 23968714
-
Clinical aspects of left ventricular diastolic function assessed by Doppler echocardiography following acute myocardial infarction.Dan Med Bull. 2001 Nov;48(4):199-210. Dan Med Bull. 2001. PMID: 11767125 Review.
-
Exercise hemodynamics in patients with and without diastolic dysfunction and preserved ejection fraction after myocardial infarction.Circ Heart Fail. 2012 Jul 1;5(4):444-51. doi: 10.1161/CIRCHEARTFAILURE.112.967919. Epub 2012 Jun 15. Circ Heart Fail. 2012. PMID: 22705767
-
Left Atrial Remodeling and Atrioventricular Coupling in a Canine Model of Early Heart Failure With Preserved Ejection Fraction.Circ Heart Fail. 2016 Oct;9(10):e003238. doi: 10.1161/CIRCHEARTFAILURE.115.003238. Epub 2016 Oct 10. Circ Heart Fail. 2016. PMID: 27758811 Free PMC article.
-
Correlation with invasive left ventricular filling pressures and prognostic relevance of the echocardiographic diastolic parameters used in the 2016 ESC heart failure guidelines and in the 2016 ASE/EACVI recommendations: a systematic review in patients with heart failure with preserved ejection fraction.Eur J Heart Fail. 2018 Sep;20(9):1303-1311. doi: 10.1002/ejhf.1220. Epub 2018 Jun 7. Eur J Heart Fail. 2018. PMID: 29877602
Cited by
-
Characterizing heart failure in the ventricular volume domain.Clin Med Insights Cardiol. 2015 Feb 25;9(Suppl 1):11-31. doi: 10.4137/CMC.S18744. eCollection 2015. Clin Med Insights Cardiol. 2015. PMID: 25780344 Free PMC article. Review.
-
Animal models of dyssynchrony.J Cardiovasc Transl Res. 2012 Apr;5(2):135-45. doi: 10.1007/s12265-011-9336-5. Epub 2011 Dec 1. J Cardiovasc Transl Res. 2012. PMID: 22130900 Free PMC article. Review.
-
Left Ventricle-Arterial System Interaction in Heart Failure.Clin Med Insights Cardiol. 2015 Jun 23;9(Suppl 1):93-9. doi: 10.4137/CMC.S18742. eCollection 2015. Clin Med Insights Cardiol. 2015. PMID: 26124691 Free PMC article. Review.
-
Left ventricular volume regulation in heart failure with preserved ejection fraction.Physiol Rep. 2013 Jul;1(2):e0007. doi: 10.1002/phy2.7. Epub 2013 Jun 26. Physiol Rep. 2013. PMID: 24303121 Free PMC article.
-
Enhanced resistance to permeability transition in interfibrillar cardiac mitochondria in dogs: effects of aging and long-term aldosterone infusion.Am J Physiol Heart Circ Physiol. 2013 Feb 15;304(4):H514-28. doi: 10.1152/ajpheart.00674.2012. Epub 2012 Dec 15. Am J Physiol Heart Circ Physiol. 2013. PMID: 23241318 Free PMC article.
References
-
- Paulus WJ, Tschope C, Sanderson JE, Rusconi C, Flachskampf FA, Rademakers FE, Marino P, Smiseth OA, De Keulenaer G, Leite-Moreira AF, Borbély A, Edes I, Handoko ML, Heymans S, Pezzali N, Pieske B, Dickstein K, Fraser AG, Brutsaert DL. How to diagnose diastolic heart failure: a consensus statement on the diagnosis of heart failure with normal left ventricular ejection fraction by the Heart Failure and Echocardiography Associations of the European Society of Cardiology. Eur Heart J. 2007;28:2539–2550. doi: 10.1093/eurheartj/ehm037. - DOI - PubMed
-
- Moller JE, Brendorp B, Ottesen M, Kober L, Egstrup K, Poulsen SH, Torp-Pedersen C. Bucindolol Evaluation in Acute Myocardial Infarction Trail Group. Congestive heart failure with preserved left ventricular systolic function after acute myocardial infarction: clinical and prognostic implications. Eur J Heart Fail. 2003;5:811–819. doi: 10.1016/S1388-9842(03)00159-4. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
