

Cardiotoxicity of anthracycline agents for the treatment of cancer: systematic review and meta-analysis of randomised controlled trials
- PMID: 20587042
- PMCID: PMC2907344
- DOI: 10.1186/1471-2407-10-337
Cardiotoxicity of anthracycline agents for the treatment of cancer: systematic review and meta-analysis of randomised controlled trials
Abstract
Background: We conducted a systematic review and meta-analysis to clarify the risk of early and late cardiotoxicity of anthracycline agents in patients treated for breast or ovarian cancer, lymphoma, myeloma or sarcoma.
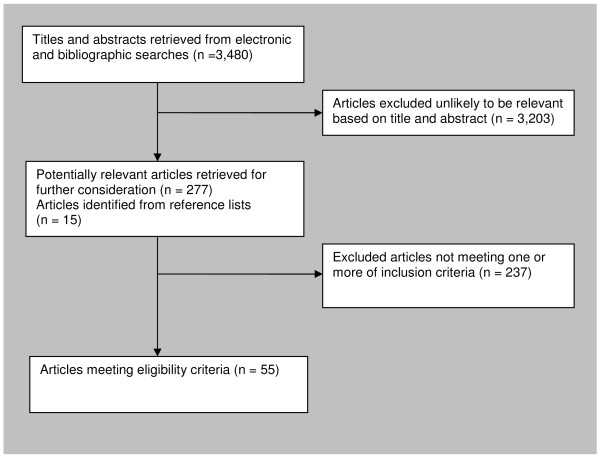
Methods: Randomized controlled trials were sought using comprehensive searches of electronic databases in June 2008. Reference lists of retrieved articles were also scanned for additional articles. Outcomes investigated were early or late clinical and sub-clinical cardiotoxicity. Trial quality was assessed, and data were pooled through meta-analysis where appropriate.
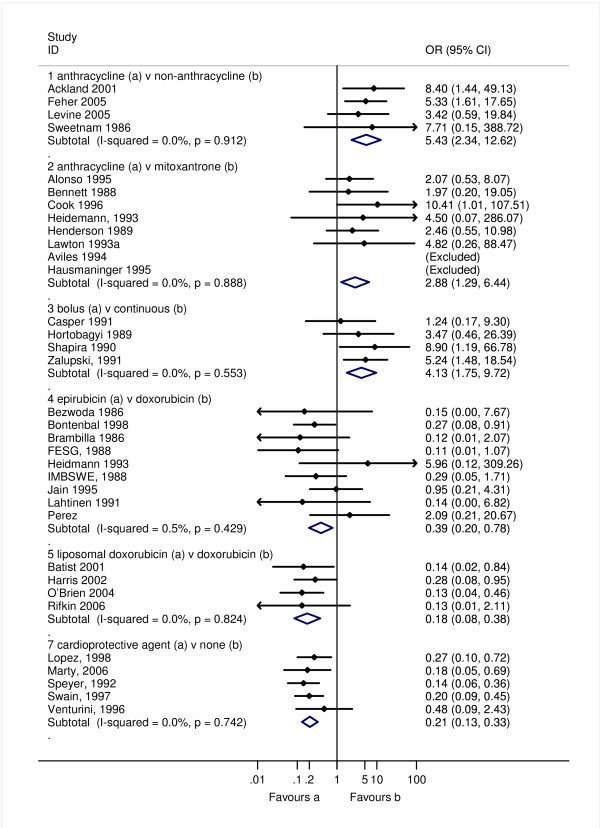
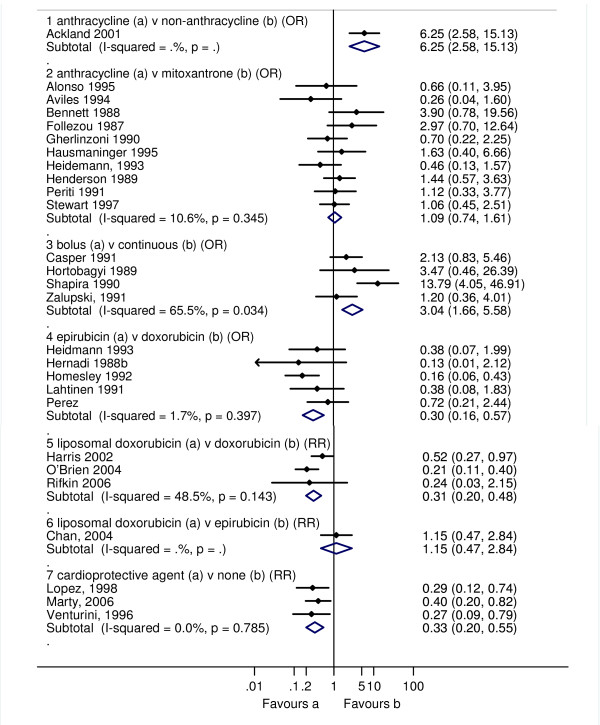
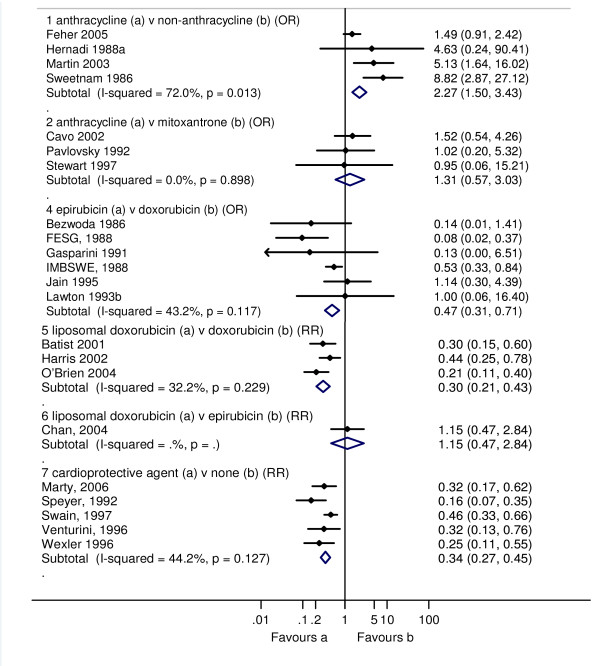
Results: Fifty-five published RCTs were included; the majority were on women with advanced breast cancer. A significantly greater risk of clinical cardiotoxicity was found with anthracycline compared with non-anthracycline regimens (OR 5.43 95% confidence interval: 2.34, 12.62), anthracycline versus mitoxantrone (OR 2.88 95% confidence interval: 1.29, 6.44), and bolus versus continuous anthracycline infusions (OR 4.13 95% confidence interval: 1.75, 9.72). Risk of clinical cardiotoxicity was significantly lower with epirubicin versus doxorubicin (OR 0.39 95% confidence interval: 0.20, 0.78), liposomal versus non-liposomal doxorubicin (OR 0.18 95% confidence interval: 0.08, 0.38) and with a concomitant cardioprotective agent (OR 0.21 95% confidence interval: 0.13, 0.33). No statistical heterogeneity was found for these pooled analyses. A similar pattern of results were found for subclinical cardiotoxicity; with risk significantly greater with anthracycline containing regimens and bolus administration; and significantly lower risk with epirubicin, liposomal doxorubicin versus doxorubicin but not epirubicin, and with concomitant use of a cardioprotective agent. Low to moderate statistical heterogeneity was found for two of the five pooled analyses, perhaps due to the different criteria used for reduction in Left Ventricular Ejection Fraction. Meta-analyses of any cardiotoxicity (clinical and subclinical) showed moderate to high statistical heterogeneity for four of five pooled analyses; criteria for any cardiotoxic event differed between studies. Nonetheless the pattern of results was similar to those for clinical or subclinical cardiotoxicity described above.
Conclusions: Evidence is not sufficiently robust to support clear evidence-based recommendations on different anthracycline treatment regimens, or for routine use of cardiac protective agents or liposomal formulations. There is a need to improve cardiac monitoring in oncology trials.
Figures
References
-
- Mulrooney DA, Yeazel MW, Kawashima T, Mertens AC, Mitby P, Stovall M, Donaldson SS, Green DM, Sklar CA, Robison LL, Leisenring WM. Cardiac outcomes in a cohort of adult survivors of childhood and adolescent cancer: retrospective analysis of the Childhood Cancer Survivor Study cohort. BMJ. 2009;339:b4606. doi: 10.1136/bmj.b4606. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
