

Clinical results of percutaneous transluminal angioplasty and stenting for intracranial vertebrobasilar atherosclerotic stenoses and occlusions
- PMID: 20587244
- PMCID: PMC3522215
- DOI: 10.1177/15910199040100S205
Clinical results of percutaneous transluminal angioplasty and stenting for intracranial vertebrobasilar atherosclerotic stenoses and occlusions
Abstract
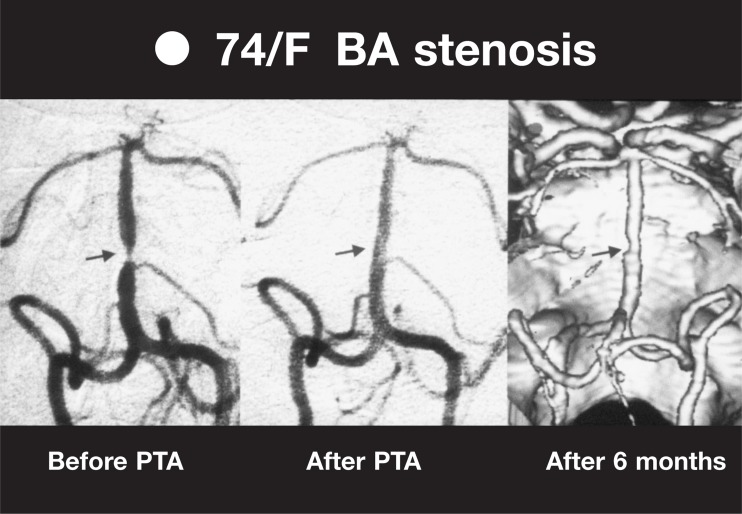
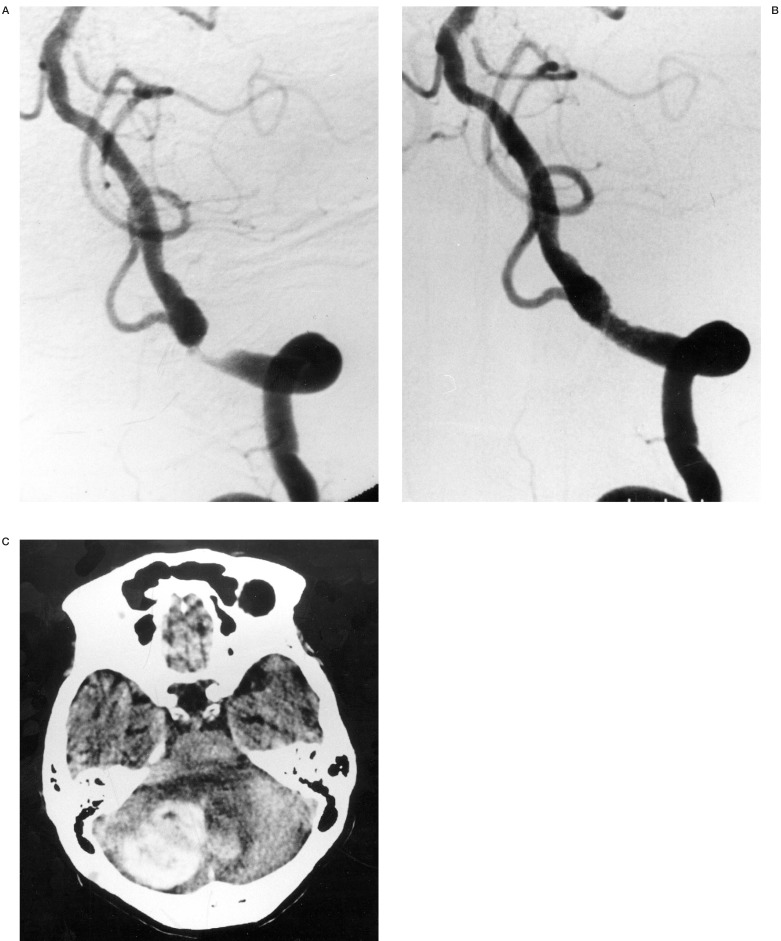
Eighteen patients with intracranial vertebrobasilar stenosis and occlusion were treated by PTA or stenting. In 11 of 18 cases, only PTA was performed and in seven of 18 cases, we used stents. The mean stenosis before and after PTA/stenting was 82.8% and 22.3%, respectively. In 11 cases of PTA only, the stenotic rate decreased from 81.8% to 29.6%, while 85.0% of the stenotic rate remarkably reduced to 6.0% in seven cases of stenting. The 30 days morbidity and 30 days mortality rate were 5.5% and 5.5%, respectively. There was only one haemorrhagic complication (cerebellar haemorrhage) in cases of stenting, and no ischemic events during or after the procedures. Restenosis (more than 50% stenosis) occurred in four of 18 cases(22.2%) during mean followup period of 12 months. Two patients with VA occlusion before treatment, developed restenosis and reocclusion. Complete total occlusion seems to be a high-risk lesion and strict follow-up is required. In this study, PTA/stenting for intracranial vertebrobasilar artery stenosis or occlusion is an effective treatment, but strict indications may be required because procedure-related 30 days morbidity rate was 5.5% in addition to unclear natural history.
Figures
References
-
- The Warfarin-Aspirin Symptomatic Intracranial Disease (WASID) Study Group. Prognosis of patients with symptomatic vertebral or basilar artery stenosis. Stroke. 1998;29:1389–1392. - PubMed
-
- Qureshi AI, Suri MFK, et al. Stroke-free survival and its determinants in patients with symptomatic vertebrobasilar stenosis: a multicenter study. Neurosurgery. 2003;52:1033–1040. - PubMed
-
- Hopkins LN, Budny JL, et al. Complications of intracranial bypass for vertebrobasilar insufficiency. J Neurosurg. 1989;70:207–211. - PubMed
-
- Rasmussen PA, Perl II J, et al. Stent-assisted angioplasty of intracranial vertebrobasilar atherosclerosis: an initial experience. J Neurosurg. 2000;92:771–778. - PubMed
LinkOut - more resources
Full Text Sources
