

Fibered electrolytically detachable platinum coils used for the endovascular treatment of intracranial aneurysms. Initial experiences and mid-term results in 474 aneurysms
- PMID: 20587260
- PMCID: PMC3463388
- DOI: 10.1177/159101990401000101
Fibered electrolytically detachable platinum coils used for the endovascular treatment of intracranial aneurysms. Initial experiences and mid-term results in 474 aneurysms
Abstract
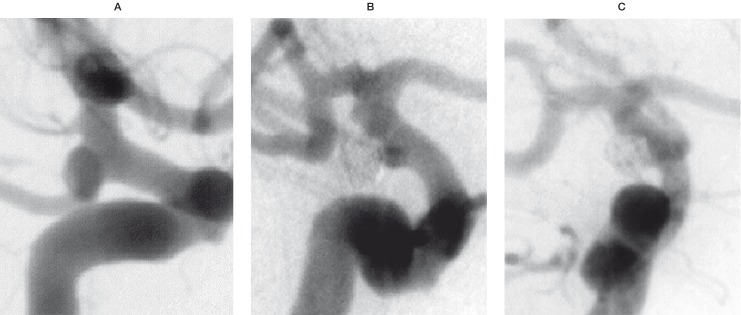
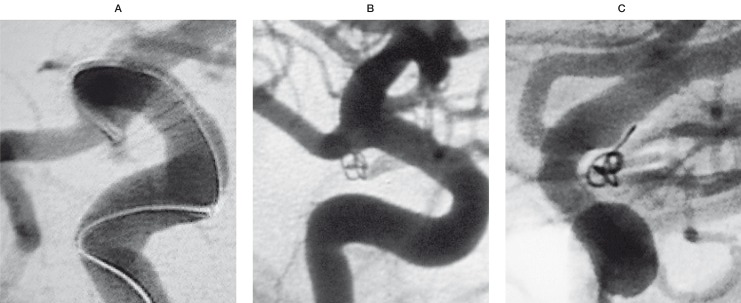
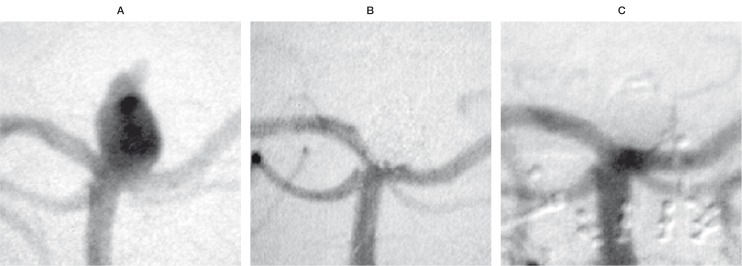
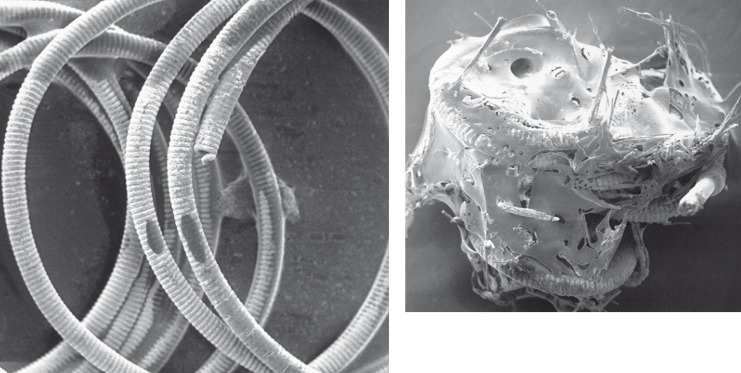
Between 1992 and 2003, a total of 2029 aneurysms in 1748 patients were treated by endovascular occlusion with electrolytically detachable coils. In this series, electrolytically detachable platinum coils with Nylon fibers (Sapphire Detachable Coil System, MTI, Irvine, CA, USA) were used in 474 aneurysms solely or in combination with bare coils from various manufacturers. To determine the safety and clinical efficacy of Nylon fibered coils for the endovascular treatment of intracranial aneurysms in comparison to bare platinum coils a thorough retrospective statistical analysis by means of logistic regression and matched pairs analysis was performed. Only treatments with data for all matching variables were used, resulting in 421 matched pairs. The analysis was performed with respect to clinical status and numerous parameters concerning individual aneurysm characteristics (e.g., location, neck width, fundus diameter). Treatment-related parameters included the use and percentage of fibered coils, occlusion rate, procedural complications, early clinical outcome and Glasgow Outcome Scale (GOS) scores. Finally, long-term follow-up results (particularly recurrence, cause of recurrence and post treatment haemorrhage) were evaluated. Both logistic regression and matched pairs analysis showed a statistically improved occlusion rate if fibered coils had been used (96% largely occluded with the use of fibered coils vs. 84-85% with the exclusive use of bare coils). However, the amount of fibered coils calculated as percentage of coil length did not seem to have significant impact. Procedures with fibered coils did not lead to a higher rate of thromboembolic events (8.0% for fibered vs. 10.5% for bare coils).The apparently better clinical outcome in the group treated with fibered coils determined by both postprocedural outcome and GOS, did not reach statistical significance. Analysis of the anatomical properties showed no differences between the groups treated with bare and fibered coils in terms of neck width, fundus diameter, and anatomic location. As expected, a higher occlusion rate was achieved in aneurysms with smaller neck and fundus independent from the type of coil used. On follow up angiography, there was an apparently lower rate of recurrence secondary to coil compaction in the group treated with fibered coils, but these data were compromised by the fact that up to date only about one third of 474 aneurysms treated with fibered coils had undergone angiographic follow-up and this did not reach statistical significance. From our experiences, we conclude that the use of fibered electrolytically detachable platinum coils in aneurysm treatment leads to significantly improved occlusion rates compared to the sole use of bare platinum coils. We hope that with increasing follow-up data we will be able to confirm that the apparently reduced recurrence rates for aneurysms treated with fibered coils can be proven with statistical significance.
Figures
Similar articles
-
Complex shaped detachable platinum coil system for the treatment of cerebral aneurysms: the Codman Trufill DCS and Trufill DCS Orbit Detachable Coil System COMPLEX Registry final results.J Neurointerv Surg. 2013 Jan 1;5(1):54-61. doi: 10.1136/neurintsurg-2011-010118. Epub 2011 Nov 4. J Neurointerv Surg. 2013. PMID: 22058182
-
In vitro and in vivo Studies of the Extent of Electrothrombotic Deposition of Blood Elements on the Surface of Electrolytically Detachable Coils.Interv Neuroradiol. 2004 Sep 30;10(3):189-201. doi: 10.1177/159101990401000301. Epub 2005 Jan 5. Interv Neuroradiol. 2004. PMID: 20587231 Free PMC article.
-
Mid-term outcome of intracranial aneurysms treated with HydroSoft coils compared to historical controls treated with bare platinum coils: a single-center experience.Acta Neurochir (Wien). 2014 Sep;156(9):1687-94. doi: 10.1007/s00701-014-2157-y. Epub 2014 Jul 1. Acta Neurochir (Wien). 2014. PMID: 24975277
-
Selection of cerebral aneurysms for treatment using Guglielmi detachable coils: the preliminary University of Illinois at Chicago experience.Neurosurgery. 1998 Dec;43(6):1281-95; discussion 1296-7. doi: 10.1097/00006123-199812000-00011. Neurosurgery. 1998. PMID: 9848841 Review.
-
Follow-up angiography of intracranial aneurysms treated with endovascular placement of Guglielmi detachable coils.Neurosurgery. 2002 Feb;50(2):239-49; discussion 249-50. doi: 10.1097/00006123-200202000-00003. Neurosurgery. 2002. PMID: 11844258 Review.
Cited by
-
Resolution of mass effect and compression symptoms following endoluminal flow diversion for the treatment of intracranial aneurysms.AJNR Am J Neuroradiol. 2013 May;34(5):935-9. doi: 10.3174/ajnr.A3547. Epub 2013 Mar 14. AJNR Am J Neuroradiol. 2013. PMID: 23493889 Free PMC article. Clinical Trial.
-
The Common but Complicated Tool: Review of Embolic Materials for the Interventional Radiologist.Semin Intervent Radiol. 2021 Nov 24;38(5):535-541. doi: 10.1055/s-0041-1736658. eCollection 2021 Dec. Semin Intervent Radiol. 2021. PMID: 34853499 Free PMC article. Review.
-
Emerging Embolic Agents in Endovascular Embolization: An Overview.Prog Biomed Eng (Bristol). 2020 Jan;2(1):012003. doi: 10.1088/2516-1091/ab6c7d. Epub 2020 Feb 12. Prog Biomed Eng (Bristol). 2020. PMID: 34553126 Free PMC article. No abstract available.
-
Advances in Biomaterials and Technologies for Vascular Embolization.Adv Mater. 2019 Aug;31(33):e1901071. doi: 10.1002/adma.201901071. Epub 2019 Jun 6. Adv Mater. 2019. PMID: 31168915 Free PMC article. Review.
-
Endovascular coiling of cerebral aneurysms using "bioactive" or coated-coil technologies: a systematic review of the literature.AJNR Am J Neuroradiol. 2009 Feb;30(2):219-26. doi: 10.3174/ajnr.A1324. Epub 2008 Oct 8. AJNR Am J Neuroradiol. 2009. PMID: 18842754 Free PMC article.
References
-
- Piton J, Billerey J, et al. Embolization par courant électrique continu: ECEC. Application thérapeutic. J Radiol. 1979;80:799–808. - PubMed
-
- Guglielmi G, Vifluela F, et al. Electrothrombosis of saccular aneurysms via endovascular approach. Part 1: Electrochemical basis, technique and experimental results. J Neurosurg. 1991;75:1–7. - PubMed
-
- Guglielmi G, Vifluela F, et al. Electrothrombosis of saccular aneurysms via endovascular approach. Part 2: Preliminary clinical experience. J Neurosurg. 1991;75:8–14. - PubMed
-
- Anonymous, (International Subarachnoid Aneurysm Trial - ISAT Collaborative Group) International Sub- arachnoid Aneurysm Trial (ISAT) of neurosurgical clipping versus endovascular coiling in 2143 patients with ruptured intracranial aneurysms: a randomised trial. Lancet. 2002;360:1267–1274. - PubMed
-
- Murayama Y, Nien YL, et al. Guglielmi detachable coil embolization of cerebral aneurysms: 11 years' experience. J Neurosurg. 2003;98:959–966. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
