

Study of Dural Arteriovenous Fistula Drains into Leptomeningeal Vein without Sinus Interposition
- PMID: 20587288
- PMCID: PMC3490160
- DOI: 10.1177/15910199040100S122
Study of Dural Arteriovenous Fistula Drains into Leptomeningeal Vein without Sinus Interposition
Abstract
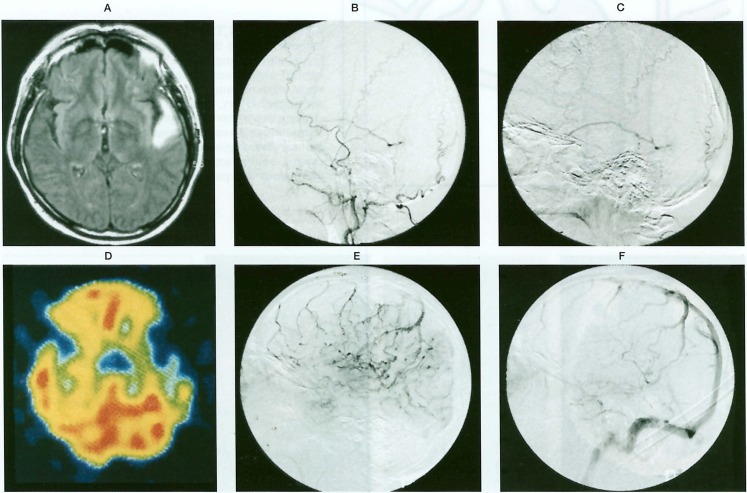
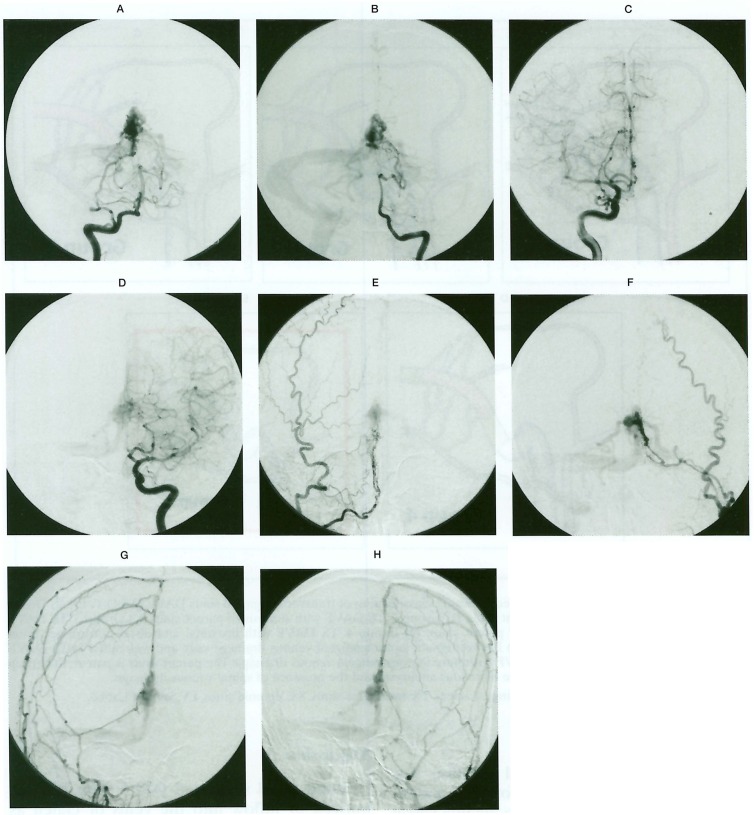
We evaluated dural arteriovenous fistulas (DAVF) drains into leptomeningeal vein (LMV) without the venous sinus interposition. This type of DAVF contained the extra-sinusal type DAVF and the DAVF with so-called pure leptomeningeal venous drainage (PLMVD).We studied 15 patients with DAVF that flows into LMVD without passing into the sinus. The subjects were 5 patients with DAVF in the anterior cranial fossa, 2 with DAVF in the tentorium cerebelli, and 3 with DAVF in the craniocervical junction as extra-sinusal type DAVF and 3 with DAVF in the transverse sigmoid sinus and 2 with DAVF in the superior sagittal sinus as DAVF with PLMVD. This type appears to take a very aggressive course. The arterial pressure of the shunt is directly applied to LMV, which causes bending and winding of the vein, eventually varices, inducing intracranial haemorrhage or venous ischemia in the LMV reflux area. Emergency treatment should be performed as soon as possible. Although it is recognized that interruption of the draining vein is very effective, treatment methods such as TAE, direct surgery, and g knife treatment, or their combinations should be carefully chosen for each case.
Figures





References
-
- Lasjaunias P, Chiu M, et al. Neurological manifestations of intracranial dural arteriovenous malformations. J Nuerosurg. 1986;64:724–730. - PubMed
-
- Borden JA, Wu JK, et al. A proposed classification for spinal and cranial dural arteriovenous fistulous malformations and implications for treatment. J Neurosurg. 1995;82:166–179. - PubMed
-
- Cognard C, Gobin YP, et al. Cerebral dural arteriovenous fistulas: Clinical and angiographic correlation with a revised classification of venous drainage. Radiology. 1995;194:671–680. - PubMed
-
- Collice M, D’Aliberti G, et al. Surgical interruption of leptomeningeal drainage as treatment for intracranial dural arteriovenous fistulas without dural sinus drainage. J Neurosurg. 1996;84:810–817. - PubMed
-
- Collice M, D’Aliberti G, et al. Surgical treatment of intracranial dural arteriovenous fistulae: role of venous drainage. Neurosurgery. 2000;47:56–67. - PubMed
LinkOut - more resources
Full Text Sources
