

Retreatment of cerebral aneurysms after guglielmi detachable coil embolization
- PMID: 20587295
- PMCID: PMC3490167
- DOI: 10.1177/15910199040100S129
Retreatment of cerebral aneurysms after guglielmi detachable coil embolization
Abstract
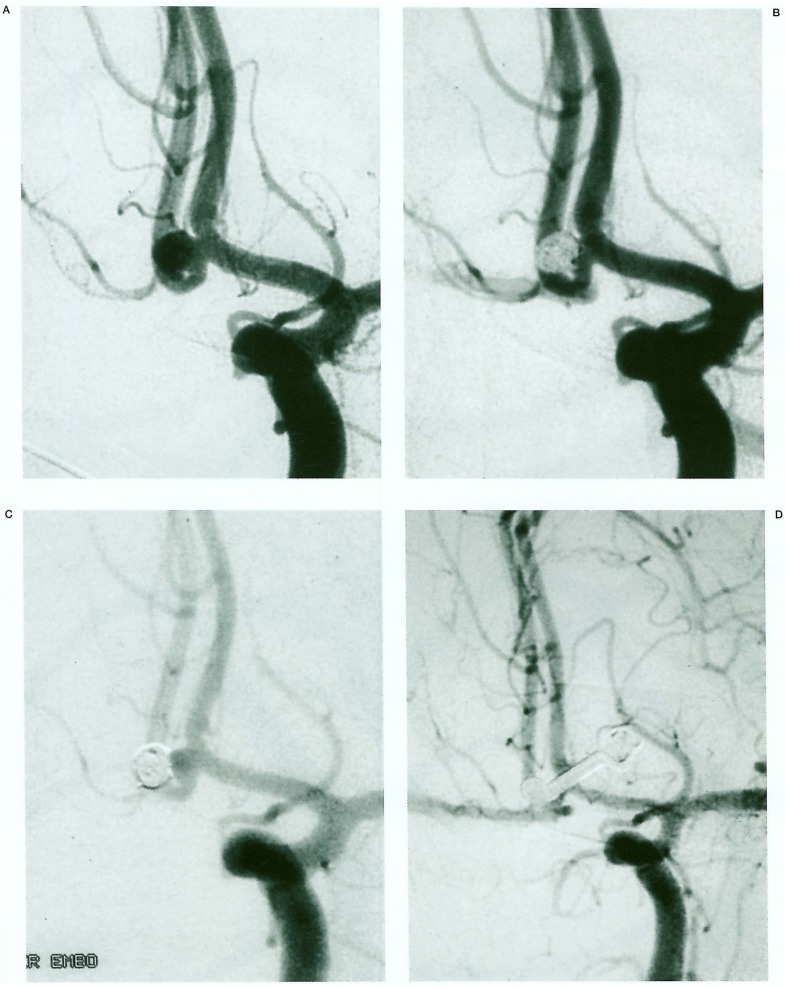
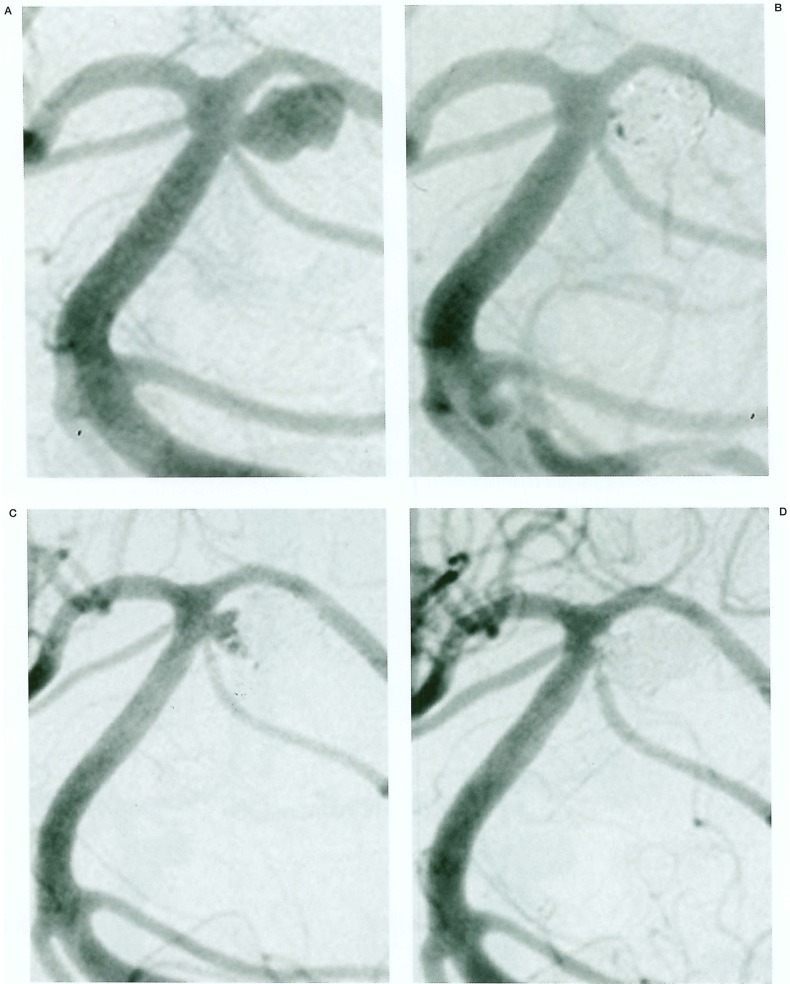
Of 175 patients with 181 aneurysms initially treated with Guglielmi Detachable Coils (GDC), 25 were retreated. All retreatments except one were performed on previously ruptured aneurysms. Thirteen aneurysms were retreated because of recurrence, and 12 aneurysms were retreated to complete initial insufficient embolization. Sixteen patients underwent re-embolization and 9 patients were operated upon surgically. No complications related to the retreatment were experienced. We consider that repeat embolization should be attempted before considering surgical treatment in case that additional therapy is required. However, it is difficult to retreat aneurysms having wide necks. In regard to surgical clipping, aneurysms without a coil in the neck are easier to treat with primary clipping, whereas aneurysms with a coil mass in the neck are difficult to surgical clip. We have never used temporary clipping and coil extraction if the distance between the coil and the parent artery was wider than 2 mm. Emerging new embolic agents or devices and technical improvement might decrease the need for retreatment and increase long-term efficacy after endovascular treatment.
Figures
References
-
- Viñuela F, Duckwiler G, et al. Guglielmi detachable coil embolization of acute intracranial aneurysm: perioperative anatomical and clinical outcome in 403 patients. J Neurosurg. 1997;86:475–482. - PubMed
-
- Raymond J, Roy D. Safety and efficacy of endovascular treatment of acutely ruptured aneurysms. Neurosurgery. 1997;41:1235–1245. - PubMed
-
- Byrne JV, Sohn MJ, et al. Five-year experience in using coil embolization for ruptured intracranial aneurysms: outcomes and incidence of late rebleeding. J Neurosurg. 1999;90:656–663. - PubMed
-
- Murayama Y, Nien YL, et al. Guglielmi detachable coil embolization of cerebral aneurysms: 11 years’ experience. J Neurosurg. 2003;98:959–966. - PubMed
-
- Molyneux A. International Subarachnoid Aneurysm Trial (ISAT) Collaborative Group: International Subarachnoid Aneurysm Trial (ISAT) of neurosurgical clipping versus endovascular coiling in 2143 patients with ruptured intracranial aneurysms: a randomised trial. Lancet. 2002;360:1267–1274. - PubMed
LinkOut - more resources
Full Text Sources
