

Should bilateral uterine artery notching be used in the risk assessment for preeclampsia, small-for-gestational-age, and gestational hypertension?
- PMID: 20587434
- PMCID: PMC3020574
- DOI: 10.7863/jum.2010.29.7.1103
Should bilateral uterine artery notching be used in the risk assessment for preeclampsia, small-for-gestational-age, and gestational hypertension?
Erratum in
- J Ultrasound Med. 2010 Oct;29(10):1494
Abstract
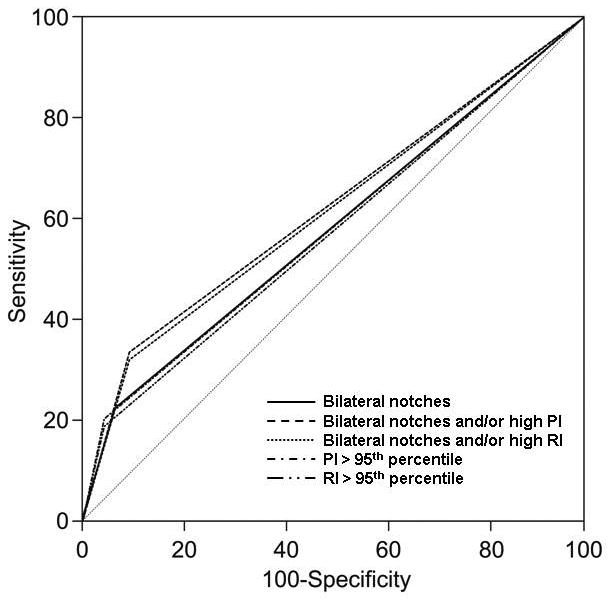
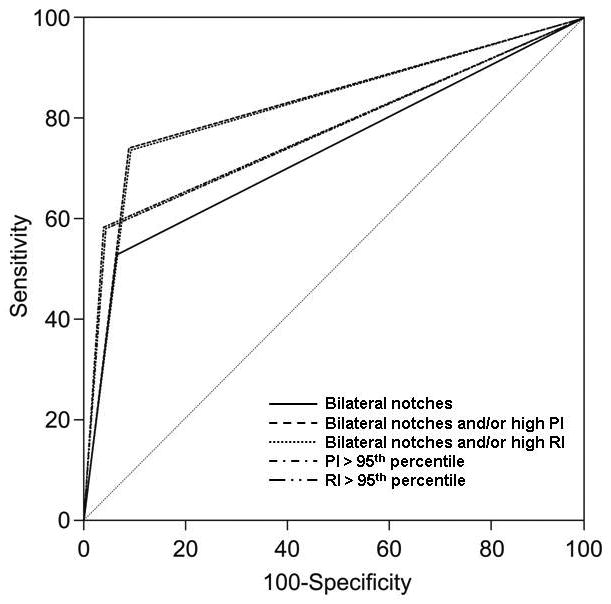
Objective: The purpose of this study was to determine the value of bilateral uterine artery notching in the second trimester in the risk assessment for preeclampsia, gestational hypertension, and small-for-gestational-age (SGA) without preeclampsia.
Methods: This prospective cohort study included 4190 singleton pregnancies that underwent ultrasound examination between 23 and 25 weeks' gestation. The 95th percentiles of the mean pulsatility index (PI) and resistive index (RI) of both uterine arteries were calculated. Multivariable logistic regression analyses were performed to determine if bilateral uterine artery notching is an independent explanatory variable for the occurrence of preeclampsia, early-onset preeclampsia (<or=34 weeks), late-onset preeclampsia (>34 weeks), gestational hypertension, and delivery of an SGA neonate without preeclampsia, while controlling for confounding factors.
Results: (1) The prevalence of preeclampsia, early-onset preeclampsia, late-onset preeclampsia, SGA, and gestational hypertension were 3.4%, 0.5%, 2.9%, 10%, and 7.9%, respectively; (2) 7.2% of the study population had bilateral uterine artery notching; and (3) bilateral uterine artery notching was an independent explanatory variable for the development of preeclampsia (odds ratio [OR], 2.1; 95% confidence interval [CI],1.28-3.36), early-onset preeclampsia (OR, 4.47; 95% CI, 1.50-13.35), and gestational hypertension (OR, 1.50; 95% CI, 1.02-2.26), but not for late-onset preeclampsia or SGA.
Conclusions: Bilateral uterine notching between 23 and 25 weeks' gestation is an independent risk factor for the development of early-onset preeclampsia and gestational hypertension. Thus, bilateral uterine artery notching should be considered in the assessment of risk for the development of these pregnancy complications.
Figures
Similar articles
-
Third trimester uterine artery Doppler indices as predictors of preeclampsia and neonatal small for gestational age.J Matern Fetal Neonatal Med. 2020 Oct;33(20):3484-3489. doi: 10.1080/14767058.2019.1575804. Epub 2019 Feb 13. J Matern Fetal Neonatal Med. 2020. PMID: 30760063
-
Comparison between three-dimensional placental volume at 12 weeks and uterine artery impedance/notching at 22 weeks in screening for pregnancy-induced hypertension, pre-eclampsia and fetal growth restriction in a low-risk population.Ultrasound Obstet Gynecol. 2006 Jun;27(6):652-7. doi: 10.1002/uog.2641. Ultrasound Obstet Gynecol. 2006. PMID: 16514618
-
Transvaginal uterine and umbilical artery Doppler examination of 12-16 weeks and the subsequent development of pre-eclampsia and intrauterine growth retardation.Ultrasound Obstet Gynecol. 1997 Feb;9(2):94-100. doi: 10.1046/j.1469-0705.1997.09020094.x. Ultrasound Obstet Gynecol. 1997. PMID: 9132263
-
First-trimester uterine artery Doppler indices in the prediction of small-for-gestational age pregnancy and intrauterine growth restriction.Ultrasound Obstet Gynecol. 2009 May;33(5):524-9. doi: 10.1002/uog.6368. Ultrasound Obstet Gynecol. 2009. PMID: 19382287
-
Third-trimester uterine artery Doppler for prediction of adverse outcome in late small-for-gestational-age fetuses: systematic review and meta-analysis.Ultrasound Obstet Gynecol. 2020 May;55(5):575-585. doi: 10.1002/uog.21940. Ultrasound Obstet Gynecol. 2020. PMID: 31785172
Cited by
-
Pre-eclampsia and the foetus: a cardiovascular perspective.Cardiovasc J Afr. 2018 Nov/Dec;29(6):387-393. doi: 10.5830/CVJA-2017-039. Cardiovasc J Afr. 2018. PMID: 31199427 Free PMC article. Review.
-
Prediction of preeclampsia and induced delivery at <34 weeks gestation by sFLT-1 and PlGF in patients with abnormal midtrimester uterine Doppler velocimetry: a prospective cohort analysis.BMC Pregnancy Childbirth. 2014 Aug 28;14:292. doi: 10.1186/1471-2393-14-292. BMC Pregnancy Childbirth. 2014. PMID: 25169665 Free PMC article.
-
Type 5 Cardiorenal Syndrome: An Underdiagnosed and Underrecognized Disease Process of the American Mother.J Clin Med Res. 2022 Oct;14(10):395-399. doi: 10.14740/jocmr4792. Epub 2022 Oct 28. J Clin Med Res. 2022. PMID: 36406945 Free PMC article. Review.
-
Umbilical Artery Doppler and Adverse Outcomes in Severe Preeclampsia Without Fetal Growth Restriction: A Retrospective Cohort Study.Cureus. 2024 Aug 26;16(8):e67850. doi: 10.7759/cureus.67850. eCollection 2024 Aug. Cureus. 2024. PMID: 39193058 Free PMC article.
-
Delayed hemolysis, elevated liver enzymes, low platelet count syndrome in succession of switches of preventive anticoagulant treatment in a 41-year-old patient with a history of recurrent assisted implantation failures: a case report.J Med Case Rep. 2019 Jan 19;13(1):16. doi: 10.1186/s13256-018-1943-1. J Med Case Rep. 2019. PMID: 30658715 Free PMC article.
References
-
- Harrington KF, Campbell S, Bewley S, Bower S. Doppler velocimetry studies of the uterine artery in the early prediction of pre-eclampsia and intra-uterine growth retardation. Eur J Obstet Gynecol Reprod Biol. 1991;42(Suppl):S14–S20. - PubMed
-
- Bower S, Bewley S, Campbell S. Improved prediction of preeclampsia by two-stage screening of uterine arteries using the early diastolic notch and color Doppler imaging. Obstet Gynecol. 1993;82:78–83. - PubMed
-
- Harrington K, Cooper D, Lees C, Hecher K, Campbell S. Doppler ultrasound of the uterine arteries: the importance of bilateral notching in the prediction of pre-eclampsia, placental abruption or delivery of a small-for-gestational-age baby. Ultrasound Obstet Gynecol. 1996;7:182–188. - PubMed
-
- Irion O, Masse J, Forest JC, Moutquin JM. Prediction of pre-eclampsia, low birthweight for gestation and prematurity by uterine artery blood flow velocity waveforms analysis in low risk nulliparous women. Br J Obstet Gynaecol. 1998;105:422–429. - PubMed
-
- Aardema MW, De Wolf BT, Saro MC, et al. Quantification of the diastolic notch in Doppler ultrasound screening of uterine arteries. Ultrasound Obstet Gynecol. 2000;16:630–634. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
