

Effects of medical therapies on retinopathy progression in type 2 diabetes
- PMID: 20587587
- PMCID: PMC4026164
- DOI: 10.1056/NEJMoa1001288
Effects of medical therapies on retinopathy progression in type 2 diabetes
Erratum in
- N Engl J Med. 2011 Jan 13;364(2):190
- N Engl J Med. 2012 Dec 20;367(25):2458
Abstract
Background: We investigated whether intensive glycemic control, combination therapy for dyslipidemia, and intensive blood-pressure control would limit the progression of diabetic retinopathy in persons with type 2 diabetes. Previous data suggest that these systemic factors may be important in the development and progression of diabetic retinopathy.
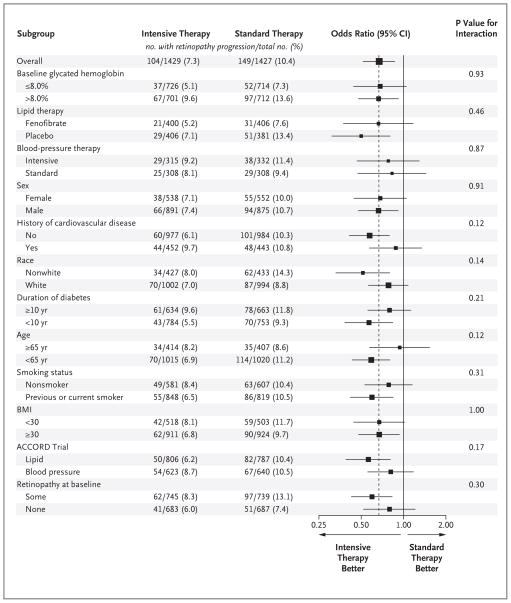
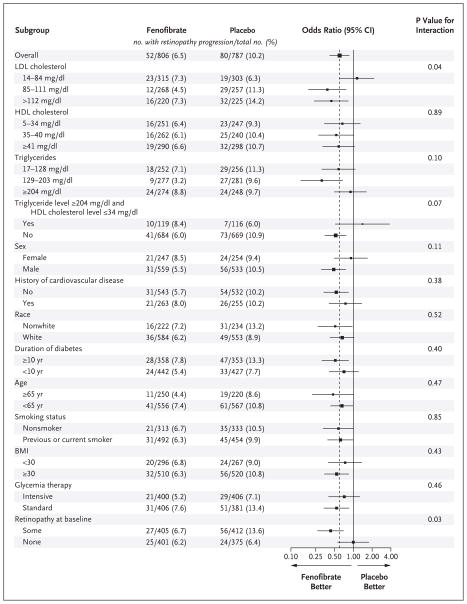
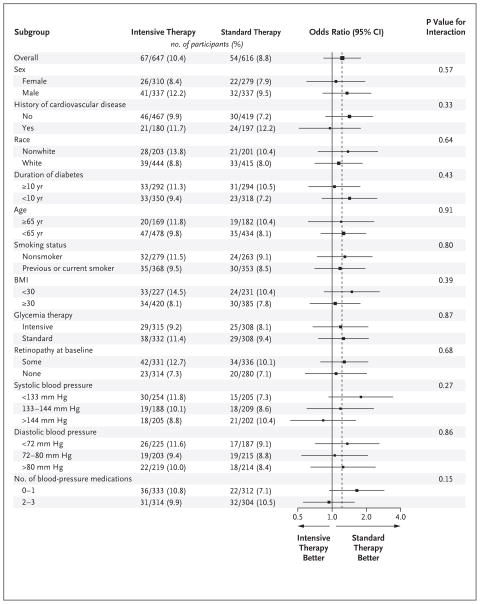
Methods: In a randomized trial, we enrolled 10,251 participants with type 2 diabetes who were at high risk for cardiovascular disease to receive either intensive or standard treatment for glycemia (target glycated hemoglobin level, <6.0% or 7.0 to 7.9%, respectively) and also for dyslipidemia (160 mg daily of fenofibrate plus simvastatin or placebo plus simvastatin) or for systolic blood-pressure control (target, <120 or <140 mm Hg). A subgroup of 2856 participants was evaluated for the effects of these interventions at 4 years on the progression of diabetic retinopathy by 3 or more steps on the Early Treatment Diabetic Retinopathy Study Severity Scale (as assessed from seven-field stereoscopic fundus photographs, with 17 possible steps and a higher number of steps indicating greater severity) or the development of diabetic retinopathy necessitating laser photocoagulation or vitrectomy.
Results: At 4 years, the rates of progression of diabetic retinopathy were 7.3% with intensive glycemia treatment, versus 10.4% with standard therapy (adjusted odds ratio, 0.67; 95% confidence interval [CI], 0.51 to 0.87; P=0.003); 6.5% with fenofibrate for intensive dyslipidemia therapy, versus 10.2% with placebo (adjusted odds ratio, 0.60; 95% CI, 0.42 to 0.87; P=0.006); and 10.4% with intensive blood-pressure therapy, versus 8.8% with standard therapy (adjusted odds ratio, 1.23; 95% CI, 0.84 to 1.79; P=0.29).
Conclusions: Intensive glycemic control and intensive combination treatment of dyslipidemia, but not intensive blood-pressure control, reduced the rate of progression of diabetic retinopathy. (Funded by the National Heart, Lung, and Blood Institute and others; ClinicalTrials.gov numbers, NCT00000620 for the ACCORD study and NCT00542178 for the ACCORD Eye study.)
2010 Massachusetts Medical Society
Conflict of interest statement
No other potential conflict of interest relevant to this article was reported.
Figures
Comment in
-
Reduction in risk of progression of diabetic retinopathy.N Engl J Med. 2010 Jul 15;363(3):287-8. doi: 10.1056/NEJMe1005667. Epub 2010 Jun 29. N Engl J Med. 2010. PMID: 20587586 No abstract available.
-
ACP Journal Club. Intensifying glucose control and adding fenofibrate to simvastatin each reduced progression of retinopathy in type 2 diabetes.Ann Intern Med. 2010 Nov 16;153(10):JC5-10. doi: 10.7326/0003-4819-153-10-201011160-02010. Ann Intern Med. 2010. PMID: 21079205 No abstract available.
-
Retinopathy progression in type 2 diabetes.N Engl J Med. 2010 Nov 25;363(22):2172-3; author reply 2173-4. doi: 10.1056/NEJMc1009236. N Engl J Med. 2010. PMID: 21105806 No abstract available.
-
Retinopathy progression in type 2 diabetes.N Engl J Med. 2010 Nov 25;363(22):2172; author reply 2173-4. doi: 10.1056/NEJMc1009236. N Engl J Med. 2010. PMID: 21105807 No abstract available.
-
Retinopathy progression in type 2 diabetes.N Engl J Med. 2010 Nov 25;363(22):2172; author reply 2173-4. doi: 10.1056/NEJMc1009236. N Engl J Med. 2010. PMID: 21105808 No abstract available.
-
Retinopathy progression in type 2 diabetes.N Engl J Med. 2010 Nov 25;363(22):2171-2; author reply 2173-4. doi: 10.1056/NEJMc1009236. N Engl J Med. 2010. PMID: 21105809 No abstract available.
-
Retinopathy progression in type 2 diabetes.N Engl J Med. 2010 Nov 25;363(22):2171; author reply 2173-4. doi: 10.1056/NEJMc1009236. N Engl J Med. 2010. PMID: 21105810 No abstract available.
-
Update of the ACCORD Eye Study.N Engl J Med. 2011 Jan 13;364(2):188-9. doi: 10.1056/NEJMc1011499. N Engl J Med. 2011. PMID: 21226603 No abstract available.
-
Fenofibrate and statin therapy, compared with placebo and statin, slows the development of retinopathy in type 2 diabetes patients of 10 years duration: the ACCORD study.Evid Based Med. 2011 Apr;16(2):45-6. doi: 10.1136/ebm1155. Evid Based Med. 2011. PMID: 21427054 No abstract available.
References
-
- Kempen JH, O’Colmain BJ, Leske MC, et al. The prevalence of diabetic retinopathy among adults in the United States. Arch Ophthalmol. 2004;122:552–63. - PubMed
-
- The effect of intensive diabetes treatment on the progression of diabetic retinopathy in insulin dependent diabetes mellitus: the Diabetes Control and Complications Trial. Arch Ophthalmol. 1995;113:36–51. - PubMed
-
- Reichard P, Nilsson BY, Rosenqvist U. The effect of long-term intensified insulin treatment on the development of microvascular complications of diabetes mellitus. N Engl J Med. 1993;329:304–9. - PubMed
-
- Ohkubo Y, Kishikawa H, Araki E, et al. Intensive insulin therapy prevents the progression of diabetic microvascular complications in Japanese patients with non-insulin-dependent diabetes mellitus: a randomized prospective 6-year study. Diabetes Res Clin Pract. 1995;28:103–17. - PubMed
-
- United Kingdom Prospective Diabetes Study Group. Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33) Lancet. 1998;352:837–53. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
- N01 HC095179/HL/NHLBI NIH HHS/United States
- N01 HC095184/HL/NHLBI NIH HHS/United States
- N01 HC095178/HC/NHLBI NIH HHS/United States
- Z99 EY999999/ImNIH/Intramural NIH HHS/United States
- N01-HC-95180/HC/NHLBI NIH HHS/United States
- N01 HC095178/HL/NHLBI NIH HHS/United States
- IAA-Y1-HC-1010/HC/NHLBI NIH HHS/United States
- N01 HC095182/HL/NHLBI NIH HHS/United States
- N01-HC-95183/HC/NHLBI NIH HHS/United States
- N01-HC-95178/HC/NHLBI NIH HHS/United States
- N01-HC-95179/HC/NHLBI NIH HHS/United States
- N01-HC-95181/HC/NHLBI NIH HHS/United States
- ZIA EY000410/ImNIH/Intramural NIH HHS/United States
- IAA-Y1-HC-9035/HC/NHLBI NIH HHS/United States
- N01 HC095180/HL/NHLBI NIH HHS/United States
- Y01 HC001010/HC/NHLBI NIH HHS/United States
- Y01 HC009035/HC/NHLBI NIH HHS/United States
- N01 HC095181/HL/NHLBI NIH HHS/United States
- N01-HC-95184/HC/NHLBI NIH HHS/United States
- R01 HL073030/HL/NHLBI NIH HHS/United States
- N01-HC-95182/HC/NHLBI NIH HHS/United States
- N01 HC095183/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases