

Immunodeficiency and the risk of serious clinical endpoints in a well studied cohort of treated HIV-infected patients
- PMID: 20588170
- PMCID: PMC2902669
- DOI: 10.1097/QAD.0b013e32833b1b26
Immunodeficiency and the risk of serious clinical endpoints in a well studied cohort of treated HIV-infected patients
Abstract
Objective: To investigate the relative predictive value of CD4(+) metrics for serious clinical endpoints.
Design: Observational.
Methods: Patients (3012; 20 317 person-years) from control arms of ESPRIT and SILCAAT were followed prospectively. We used Cox regression to identify CD4(+) metrics (latest, baseline and nadir CD4(+) cell count, latest CD4(+)%, time spent with CD4(+) count below certain thresholds and CD4(+) slopes) independently predictive of all-cause mortality, non-AIDS deaths, non-AIDS (cardiovascular, hepatic, renal and non-AIDS malignancy) and AIDS events. Akaike information criteria (AIC) were calculated for each model. Significant metrics (P < 0.05) were then additionally adjusted for latest CD4(+) cell count.
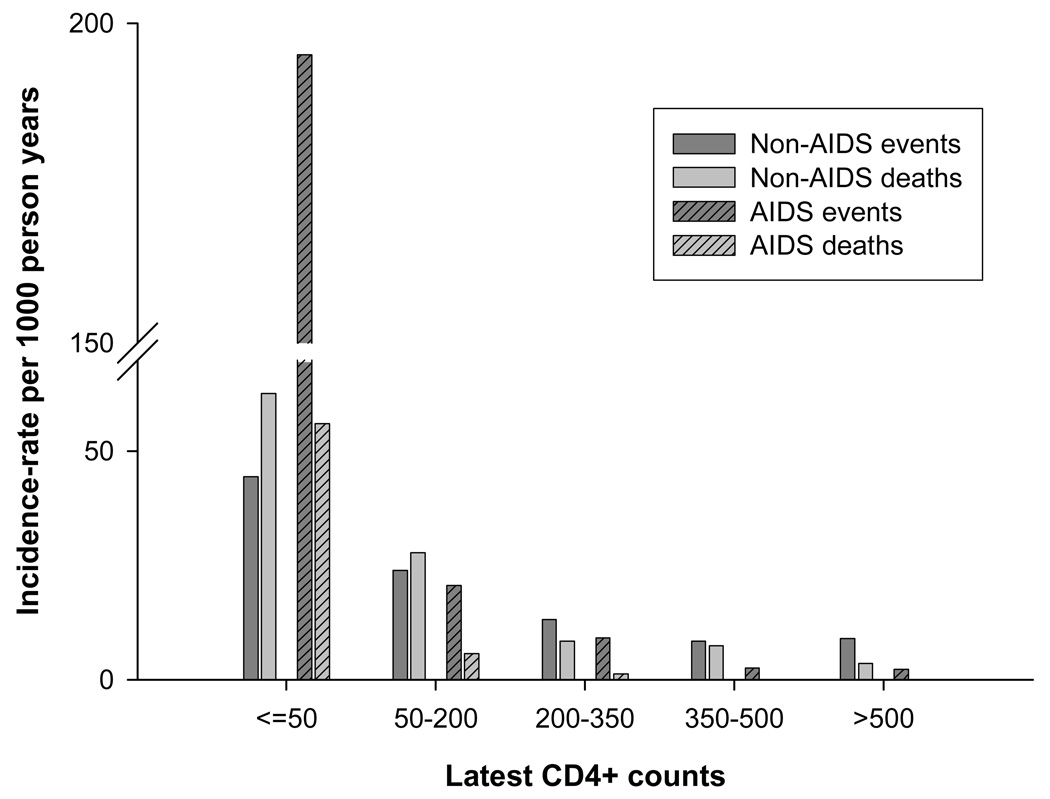
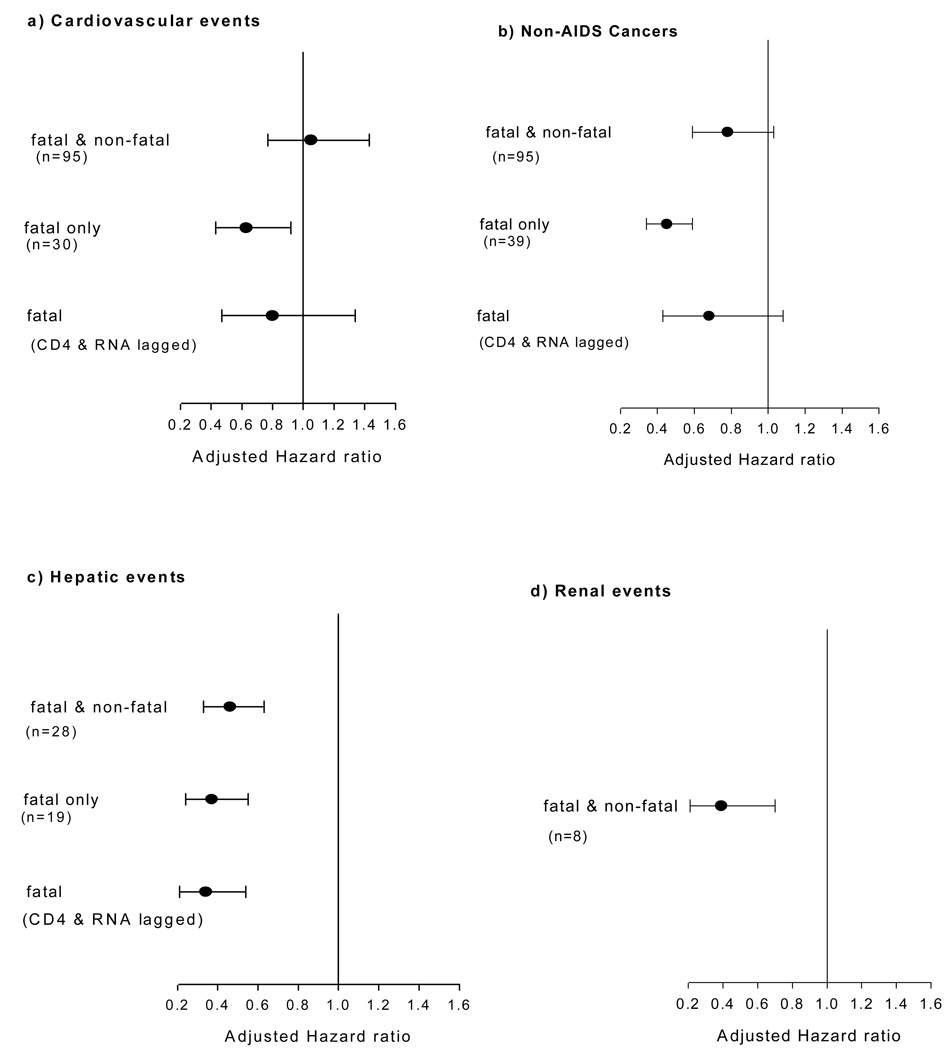
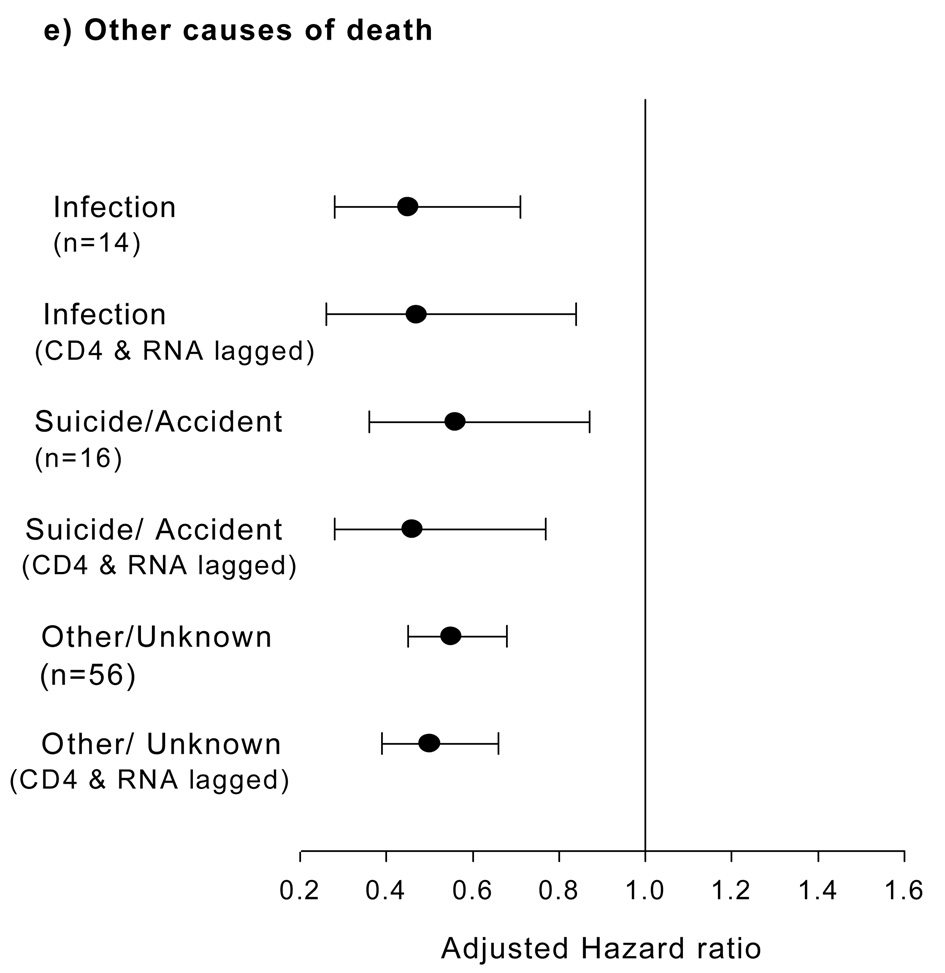
Results: Non-AIDS deaths occurred at a higher rate than AIDS deaths [rate ratio: 6.48, 95% confidence interval (CI) 5.1-8.1], and non-AIDS events likewise (rate ratio: 1.72, 95% CI 1.65-1.79). Latest CD4(+) cell count was strongly predictive of lower risk of death (hazard ratio per log2 rise: 0.48, 95% CI 0.43-0.54), with lowest AIC of all metrics. CD4(+) slope over seven visits, after additional adjustment for latest CD4(+) cell count, was the only metric to be an independent predictor for all-cause (hazard ratio for slope <-10 cells/microl per month vs. 0 +/- 10: 3.04, 95% CI 1.98-4.67) and non-AIDS deaths (hazard ratio for slope <-10 cells/microl per month vs. 0 +/- 10: 2.62, 95% CI 1.62-4.22). Latest CD4(+) cell count (per log(2) rise) was the best predictor across all four endpoints and predicted hepatic (hazard ratio 0.46, 95% CI 0.33-0.63) and renal events (hazard ratio 0.39, 95% CI 0.21-0.70), but not cardiovascular events (hazard ratio 1.05, 95% CI 0.77-1.43) or non-AIDS cancers (hazard ratio 0.78, 95% CI 0.59-1.03).
Conclusion: Latest CD4(+) cell count is the best predictor of serious endpoints. CD4(+) slope independently predicts all-cause and non-AIDS deaths.
Figures
References
-
- Mocroft A, Vella S, Benfield TL, Chiesi A, Miller V, Gargalianos P, et al. EuroSIDA Study Group. Changing patterns of mortality across Europe in patients infected with HIV-1. Lancet. 1998;352:1725–1730. - PubMed
-
- Sackoff JE, Hanna DB, Pfeiffer MR, Torian LV. Causes of death among persons with AIDS in the era of highly active antiretroviral therapy: New York City. Ann Intern Med. 2006;145:397–406. - PubMed
-
- Smit C, Geskus R, Walker S, Sabin C, Coutinho R, Porter K, et al. Effective therapy has altered the spectrum of cause-specific mortality following HIV seroconversion. AIDS. 2006;20:741–749. - PubMed
-
- Burgi A, Brodine S, Wegner S, Milazzo M, Wallace MR, Spooner K, et al. Incidence and risk factors for the occurrence of non-AIDS-defining cancers among human immunodeficiency virus-infected individuals. Cancer. 2005;104:1505–1511. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
