

Physical dependence potential of daily tramadol dosing in humans
- PMID: 20589494
- PMCID: PMC3028382
- DOI: 10.1007/s00213-010-1919-3
Physical dependence potential of daily tramadol dosing in humans
Abstract
Rationale: Tramadol is an atypical, mixed-mechanism analgesic involving both opioid and catecholamine processes that appears to have low abuse potential and may be useful as a treatment for opioid dependence.
Objectives: The current study assessed the level of physical dependence and opioid blockade efficacy produced by daily maintenance on oral tramadol.
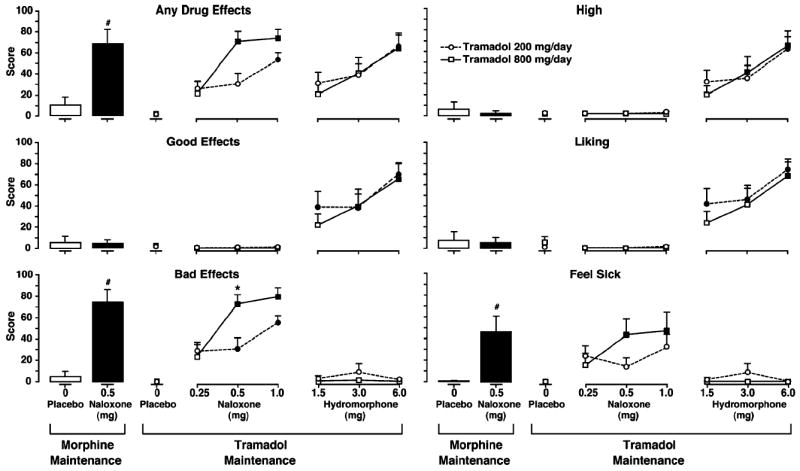
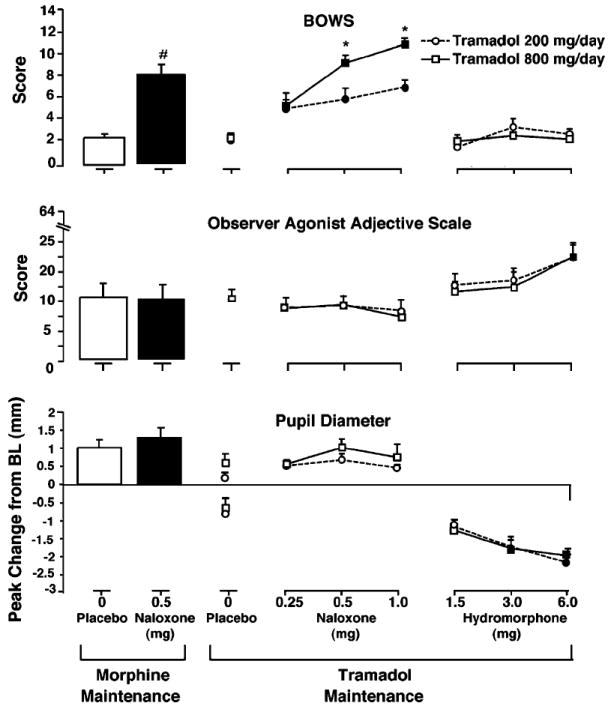
Methods: Nine residential opioid-dependent adults were maintained on two doses of daily oral tramadol (200 and 800 mg) for approximately 4-week intervals in a randomized, double-blind, crossover design. The acute effects of intramuscular placebo, naloxone (0.25, 0.5, and 1.0 mg), and hydromorphone (1.5, 3.0, and 6.0 mg) were tested under double-blind, randomized conditions. Outcomes included observer- and subject-rated measures and physiologic indices.
Results: Challenge doses of naloxone resulted in significantly higher mean peak withdrawal scores compared to placebo. Withdrawal intensity from naloxone was generally greater during 800 versus 200 mg/day tramadol maintenance. Mean peak ratings of agonist effects were elevated at higher hydromorphone challenge doses, but did not differ significantly between tramadol doses. Physiologic measures were generally affected by challenge conditions in a dose-dependent manner, with few differences between tramadol maintenance dose conditions.
Conclusions: Chronic tramadol administration produces dose-related opioid physical dependence, without producing dose-related attenuation of agonist challenge effects. Tramadol may be a useful treatment for patients with low levels of opioid dependence or as a treatment for withdrawal during opioid detoxification, but does not appear to be effective as a maintenance medication due to a lack of opioid cross-tolerance.
Conflict of interest statement
Figures
References
-
- Barsotti CE, Mycyk MB, Reyes J. Withdrawal syndrome from tramadol hydrochloride. Am J Emerg Med. 2003;21:87–88. - PubMed
-
- Cami J, Lamas X, Farre M. Acute effects of tramadol in methadone-maintained volunteers. Drugs. 1994;47(Suppl 1):39–43. - PubMed
-
- Carroll CP, Walsh SL, Bigelow GE, Strain EC, Preston KL. Assessment of agonist and antagonist effects of tramadol in opioid-dependent humans. Exp Clin Psychopharmacol. 2006;14:109–120. - PubMed
-
- Cicero TJ, Adams EH, Geller A, Inciardi JA, Munoz A, Schnoll SH, Senay EC, Woody GE. A postmarketing surveillance program to monitor Ultram (tramadol hydrochloride) abuse in the United States. Drug Alcohol Depend. 1999;57:7–22. - PubMed
-
- Cicero TJ, Inciardi JA, Adams EH, Geller A, Senay EC, Woody GE, Munoz A. Rates of abuse of tramadol remain unchanged with the introduction of new branded and generic products: results of an abuse monitoring system, 1994–2004. Pharmacoepidemiol Drug Saf. 2005;14:851–859. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
