

Three-dimensional head shape quantification for infants with and without deformational plagiocephaly
- PMID: 20590458
- PMCID: PMC2899494
- DOI: 10.1597/09-059.1
Three-dimensional head shape quantification for infants with and without deformational plagiocephaly
Abstract
Objective: The authors developed and tested three-dimensional (3D) indices for quantifying the severity of deformational plagiocephaly (DP).
Design: The authors evaluated the extent to which infants with and without DP (as determined by clinic referral and two experts' ratings) could be correctly classified.
Participants: Infants aged 4 to 11 months, including 154 with diagnosed DP and 100 infants without a history of DP or other craniofacial condition. After excluding participants with discrepant expert ratings, data from 90 infants with DP and 50 infants without DP were retained.
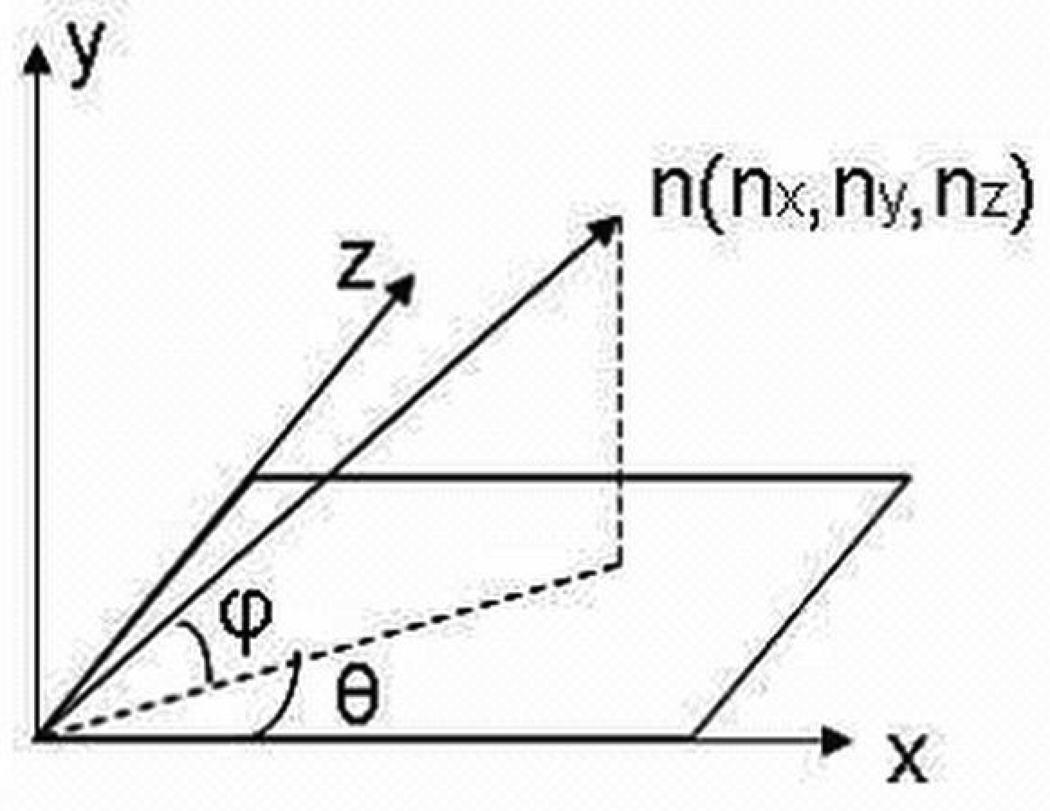
Measurements: Two-dimensional (2D) histograms of surface normal vector angles were extracted from 3D mesh data and used to compute the severity scores.
Outcome measures: Left posterior flattening score (LPFS), right posterior flattening score (RPFS), asymmetry score (AS), absolute asymmetry score (AAS), and an approximation of a previously described 2D measure, the oblique cranial length ratio (aOCLR). Two-dimensional histograms localized the posterior flatness for each participant.
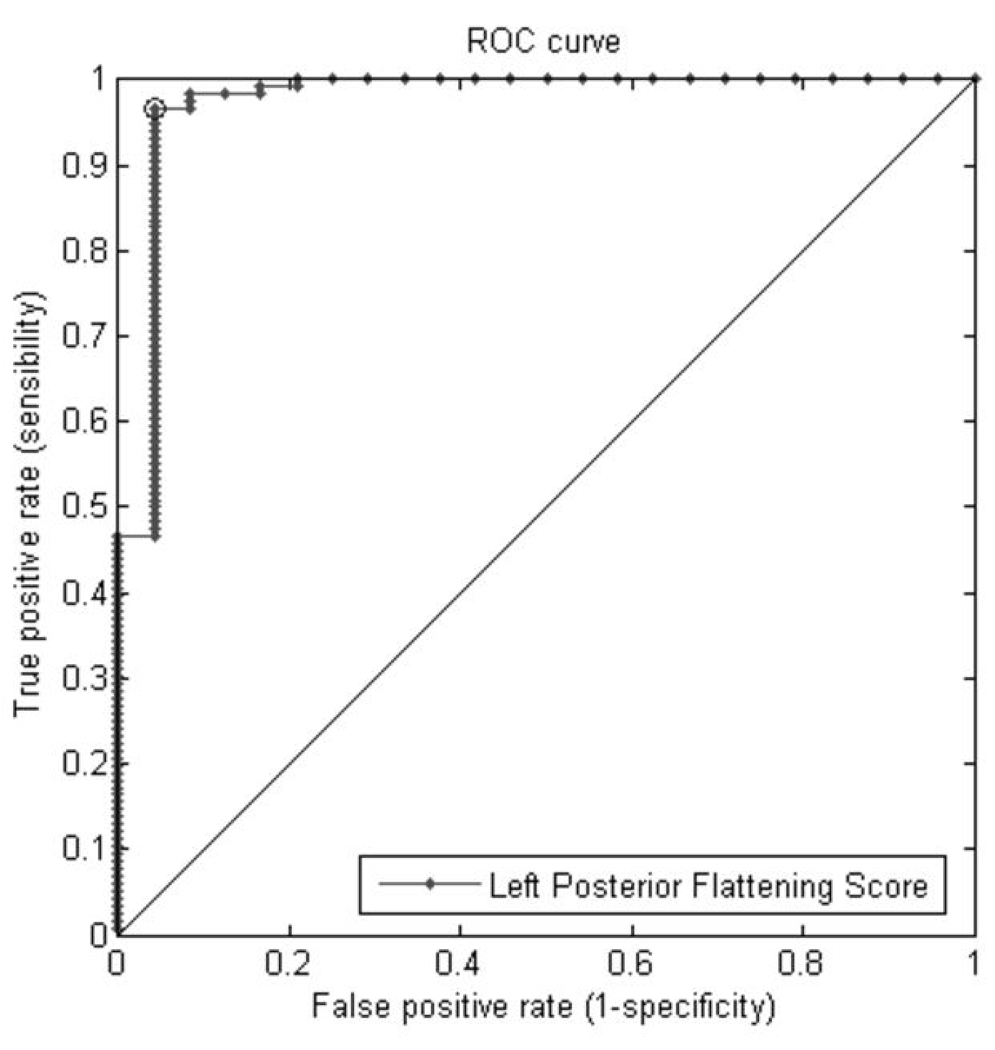
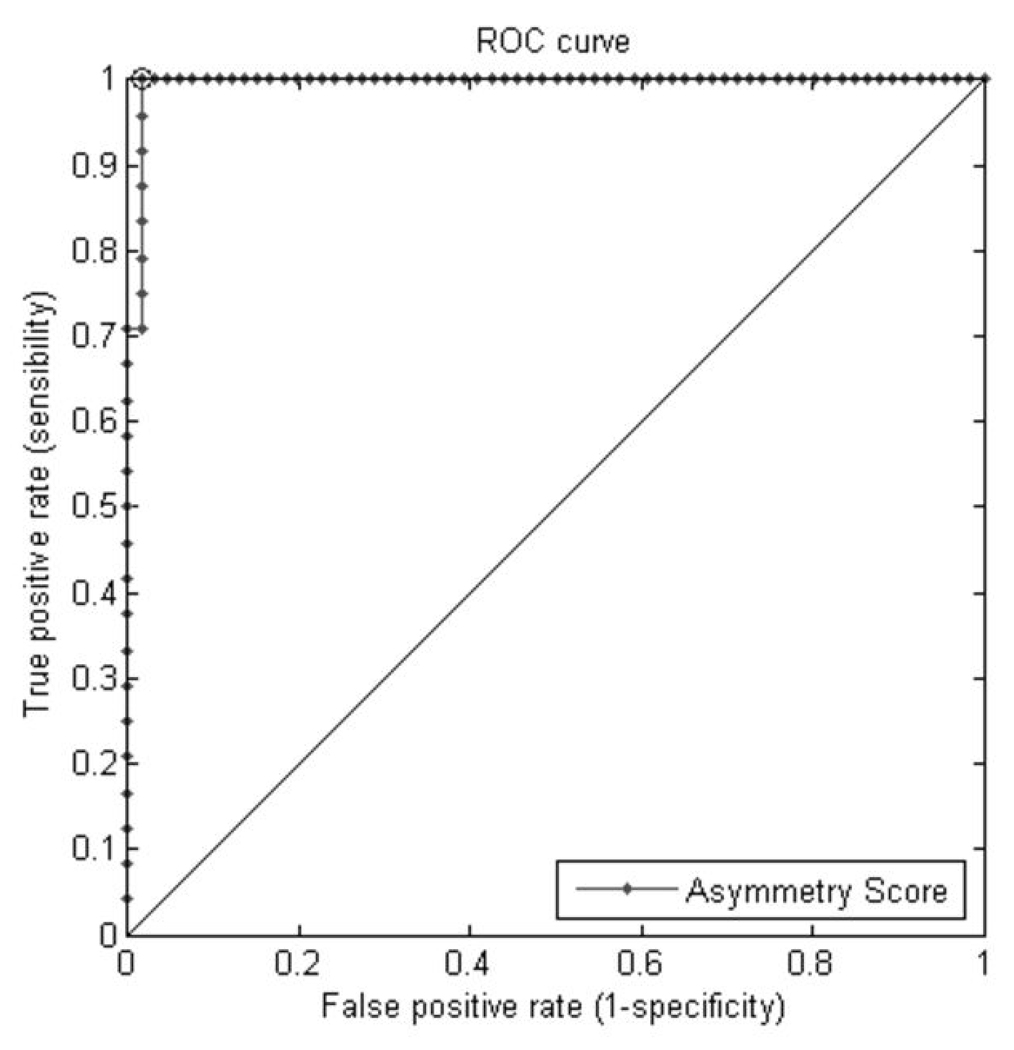
Analysis: The authors fit receiver operating characteristic curves and calculated the area under the curves (AUC) to evaluate the relative accuracy of DP classification using the above measures.
Results: The AUC statistics were AAS = 91%, LPFS = 97%, RPFS = 91%, AS = 99%, and aOCLR = 79%.
Conclusion: Novel 3D-based plagiocephaly posterior severity scores provided better sensitivity and specificity in the discrimination of plagiocephalic and typical head shapes than the 2D measurements provided by a close approximation of OCLR. These indices will allow for more precise quantification of the DP phenotype in future studies on the prevalence of this condition, which may lead to improved clinical care.
Figures













References
-
- 3-DMD. 3-DMDcranialTM System. Atlanta, GA: 2004.
-
- Argenta LC, David LR, Wilson J, Bell WO. An increase in infant cranial deformity with supine sleep positioning. J Craniofac Surg. 1996;7:5–11. - PubMed
-
- Bialocerkowski AE, Vladusic SL, Howell SM. Conservative interventions for positional plagiocephaly: a systematic review. Developmental Medicine & Child Neurology. 2005;47:563–570. - PubMed
-
- Bialocerkowski AE, Vladusic SL, Ng CW. Prevalence, risk factors, and natural history of positional plagiocephaly: A systematic review. Developmental Medicine & Child Neurolog. 2008;50:577–586. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
