

The impact of preoperative erectile dysfunction on survival after radical prostatectomy
- PMID: 20590546
- PMCID: PMC3810948
- DOI: 10.1111/j.1464-410X.2010.09472.x
The impact of preoperative erectile dysfunction on survival after radical prostatectomy
Abstract
Purpose: Erectile dysfunction (ED) and cardiovascular disease (CVD) share etiology and pathophysiology. The underlying pathology for preoperative ED may adversely affect survival following radical prostatectomy (RP). We examined the association between preoperative ED and survival following RP.
Materials and methods: Between 1983 and 2000, a single surgeon performed RP on 2511 men, with preoperative ED (ED group, n= 231, 9.2%) or without ED (No ED group, n= 2280, 90.8%). We retrospectively analysed their CVD-specific survival (CVDSS), prostate cancer-specific survival (PCSS), non-PCSS (NPCSS) and overall survival (OS) from time of surgery.
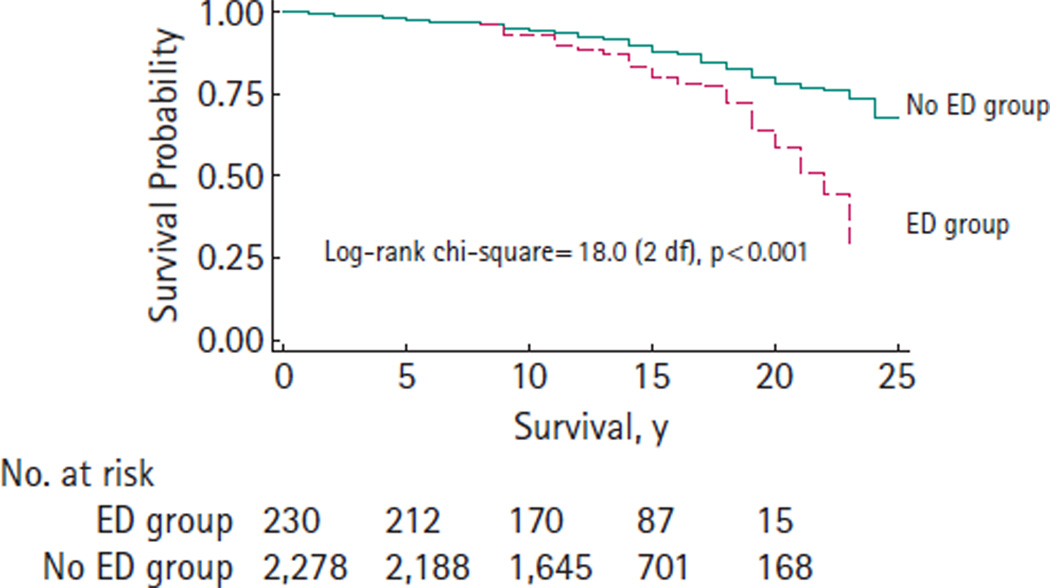
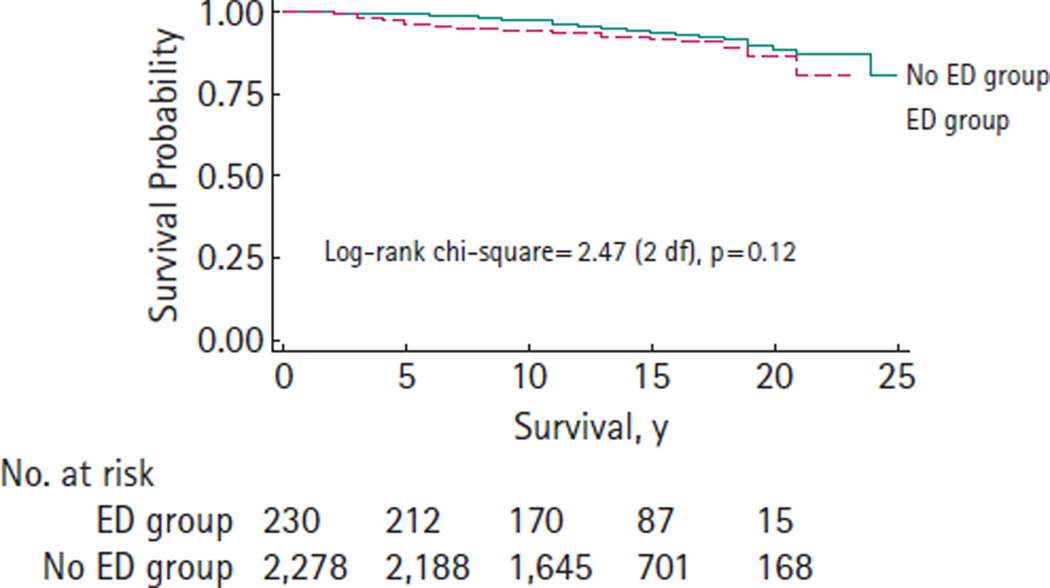
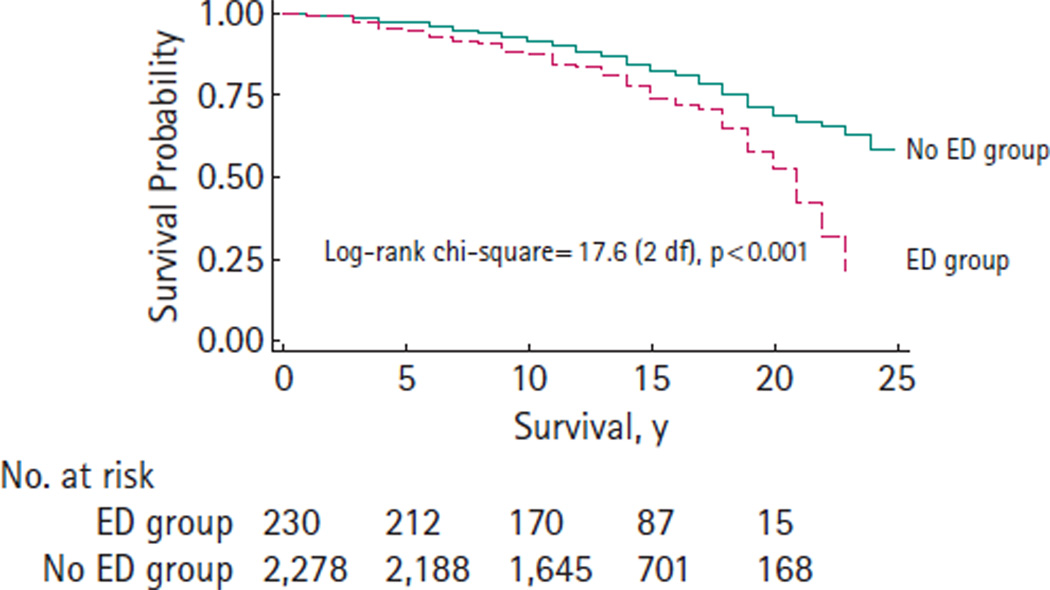
Results: With median follow-up of 13 years after RP, 449 men (18%) died (140 from prostate cancer, 309 from other causes). Kaplan-Meier analyses demonstrated significant differences in CVDSS (P < 0.001), NPCSS (P < 0.001) and OS (P < 0.001), but not in PCSS (P= 0.12), between the ED group vs No ED group. In univariate proportional hazards analyses, preoperative ED was associated with a significant decrease in OS, hazard ratio (HR), 1.71 (95% CI, 1.34-2.23), P < 0.001. However, in multivariable analyses, the association of ED with survival became non-significant (HR, 1.25 (95% CI, 0.97-1.66), P= 0.111) after adjusting for other prognostic factors, such as age, preoperative prostate-specific antigen (PSA) level, Gleason score, pathologic stage, body mass index and Charlson Comorbidity Index.
Conclusions: Preoperative ED is associated with decreased overall survival and survival from causes other than prostate cancer following RP. However, preoperative ED was not an independent predictor of overall survival after adjusting for other predictors of survival. Urologists should carefully assess pretreatment ED status to enhance appropriate treatment recommendation for men with prostate cancer.
© 2010 THE AUTHORS. JOURNAL COMPILATION © 2010 BJU INTERNATIONAL.
Conflict of interest statement
None declared. Source of funding: this study was supported in part by funds from the National Cancer Institute Grant CA58236 SPORE in Prostate Cancer, the Jahnigen Career Development from the American Geriatrics Society (M. Han) and by gifts from Dr and Mrs Peter S. Bing (B. Trock).
Figures
Similar articles
-
Association between preoperative erectile dysfunction and prostate cancer features--an analysis from the Duke Prostate Center Database.J Sex Med. 2012 Apr;9(4):1174-81. doi: 10.1111/j.1743-6109.2011.02547.x. Epub 2011 Dec 21. J Sex Med. 2012. PMID: 22188861
-
Charlson comorbidity index is an important prognostic factor for long-term survival outcomes in Korean men with prostate cancer after radical prostatectomy.Yonsei Med J. 2014 Mar;55(2):316-23. doi: 10.3349/ymj.2014.55.2.316. Yonsei Med J. 2014. PMID: 24532498 Free PMC article.
-
Long-term radical prostatectomy outcomes among participants from the European Randomized Study of Screening for Prostate Cancer (ERSPC) Rotterdam.BJU Int. 2012 Dec;110(11):1678-83. doi: 10.1111/j.1464-410X.2012.11367.x. Epub 2012 Sep 21. BJU Int. 2012. PMID: 22998182 Clinical Trial.
-
First Postprostatectomy Ultrasensitive Prostate-specific Antigen Predicts Survival in Patients with High-risk Prostate Cancer Pathology.Eur Urol Oncol. 2018 Oct;1(5):378-385. doi: 10.1016/j.euo.2018.07.008. Epub 2018 Aug 22. Eur Urol Oncol. 2018. PMID: 31158076
-
New Prostate Cancer Grading System Predicts Long-term Survival Following Surgery for Gleason Score 8-10 Prostate Cancer.Eur Urol. 2017 Jun;71(6):907-912. doi: 10.1016/j.eururo.2016.11.006. Epub 2016 Nov 19. Eur Urol. 2017. PMID: 27876305
Cited by
-
Cavernous Nerve Injury Resulted Erectile Dysfunction and Regeneration.J Immunol Res. 2021 Dec 21;2021:5353785. doi: 10.1155/2021/5353785. eCollection 2021. J Immunol Res. 2021. PMID: 34970630 Free PMC article. Review.
-
Obesity as a Risk Factor for Prostate Cancer Mortality: A Systematic Review and Dose-Response Meta-Analysis of 280,199 Patients.Cancers (Basel). 2021 Aug 19;13(16):4169. doi: 10.3390/cancers13164169. Cancers (Basel). 2021. PMID: 34439328 Free PMC article. Review.
-
Association of Obesity With Survival Outcomes in Patients With Cancer: A Systematic Review and Meta-analysis.JAMA Netw Open. 2021 Mar 1;4(3):e213520. doi: 10.1001/jamanetworkopen.2021.3520. JAMA Netw Open. 2021. PMID: 33779745 Free PMC article.
-
Body mass index and mortality in prostate cancer patients: a dose-response meta-analysis.Prostate Cancer Prostatic Dis. 2016 Jun;19(2):122-31. doi: 10.1038/pcan.2015.64. Epub 2016 Jan 12. Prostate Cancer Prostatic Dis. 2016. PMID: 26754262 Review.
-
A prediction model relating the extent of intraoperative fascia preservation to erectile dysfunction after nerve-sparing robot-assisted radical prostatectomy.J Robot Surg. 2019 Jun;13(3):455-462. doi: 10.1007/s11701-018-0867-5. Epub 2018 Sep 3. J Robot Surg. 2019. PMID: 30178300
References
-
- Han M, Partin AW, Pound CR, Epstein JI, Walsh PC. Long-term biochemical disease-free and cancer-specific survival following anatomic radical retropubic prostatectomy. The 15-year Johns Hopkins experience. Urol Clin North Am. 2001;28:555–565. - PubMed
-
- NIH Consensus Development. Panel on Impotence. NIH Consensus Conference. Impotence. JAMA. 1993;270:83–90. - PubMed
-
- Thompson IM, Tangen CM, Goodman PJ, Probstfield JL, Moinpour CM, Coltman CA. Erectile dysfunction and subsequent cardiovascular disease. JAMA. 2005;294:2996–3002. - PubMed
-
- Romano PS, Roos LL, Jollis JG. Adapting a clinical comorbidity index for use with ICD-9-CM administrative data: differing perspectives. J Clin Epidemiol. 1993;46:1075–1079. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
