

Meta-analysis of randomized controlled trials on the effectiveness of somatostatin analogues for pancreatic surgery: a Cochrane review
- PMID: 20590882
- PMCID: PMC2889267
- DOI: 10.1111/j.1477-2574.2010.00157.x
Meta-analysis of randomized controlled trials on the effectiveness of somatostatin analogues for pancreatic surgery: a Cochrane review
Abstract
Background: The use of synthetic analogues of somatostatin following pancreatic surgery is controversial. The aim of this meta-analysis is to determine whether prophylactic somatostatin analogues (SAs) should be used routinely in pancreatic surgery.
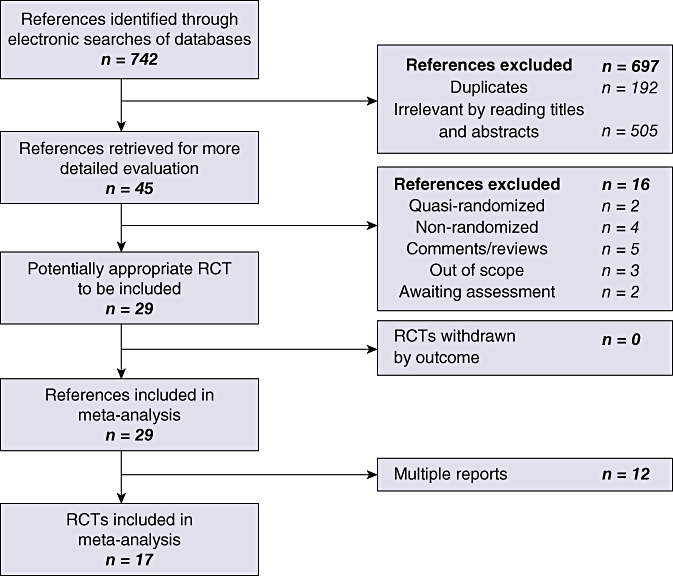
Methods: Randomized controlled trials were identified from the Cochrane Library Trials Register, MEDLINE, EMBASE, Science Citation Index Expanded and reference lists. Data were extracted from these trials by two independent reviewers. The risk ratio (RR), mean difference (MD) and standardized mean difference (SMD) were calculated with 95% confidence intervals (95% CIs) based on intention-to-treat or available case analysis.
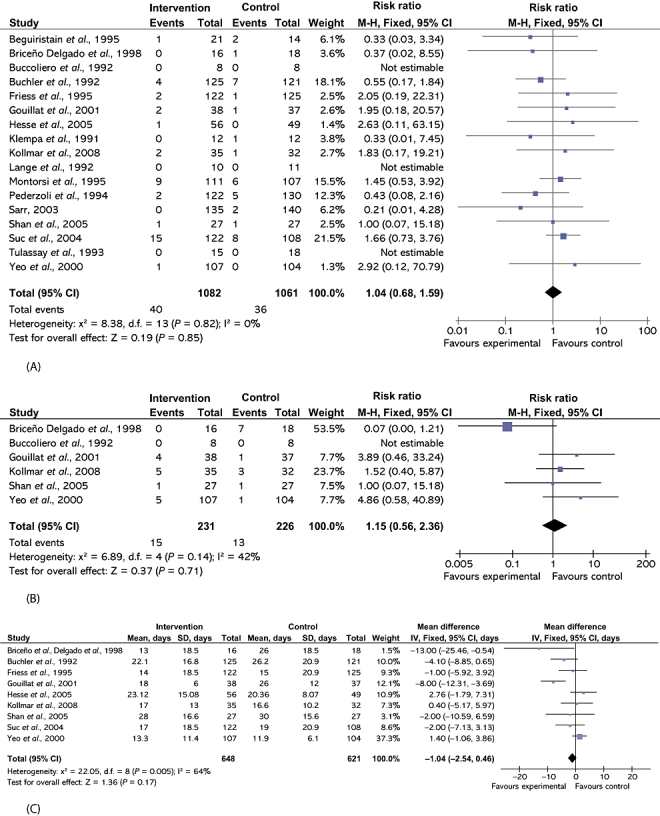
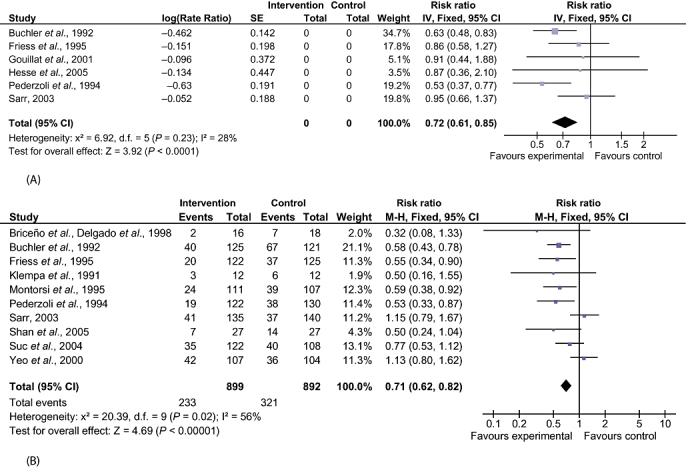
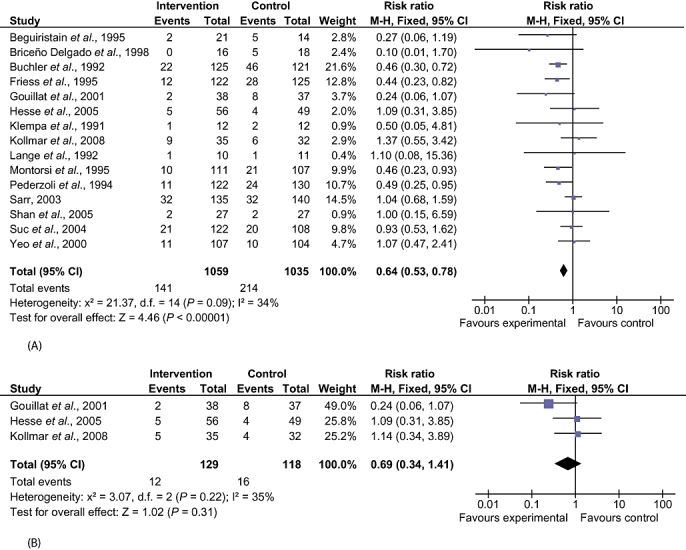
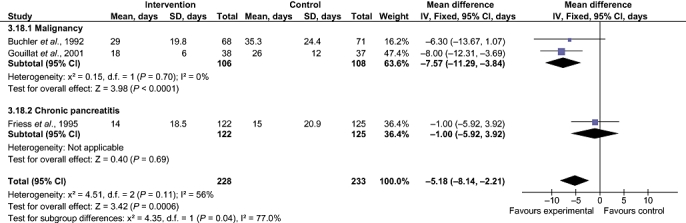
Results: Seventeen trials involving 2143 patients were identified. The overall number of patients with postoperative complications was lower in the SA group (RR 0.71, 95% CI 0.62-0.82), but there was no difference between the groups in perioperative mortality (RR 1.04, 95% CI 0.68-1.59), re-operation rate (RR 1.15, 95% CI 0.56-2.36) or hospital stay (MD -1.04 days, 95% CI -2.54 to 0.46). The incidence of pancreatic fistula was lower in the SA group (RR 0.64, 95% CI 0.53-0.78). The proportion of these fistulas that were clinically significant is not clear. Analysis of results of trials that clearly distinguished clinically significant fistulas revealed no difference between the two groups (RR 0.69, 95% CI 0.34-1.41). Subgroup analysis revealed a shorter hospital stay in the SA group than among controls for patients with malignant aetiology (MD -7.57 days, 95% CI -11.29 to -3.84).
Conclusions: Somatostatin analogues reduce perioperative complications but do not reduce perioperative mortality. However, they do shorten hospital stay in patients undergoing pancreatic surgery for malignancy. Further adequately powered trials of low risk of bias are necessary.
Figures
References
-
- Alexakis N, Halloran C, Raraty M, Ghaneh P, Sutton R, Neoptolemos JP. Current standards of surgery for pancreatic cancer. Br J Surg. 2004;91:1410–1427. - PubMed
-
- Sohn TA, Yeo CJ, Cameron JL, Koniaris L, Kaushal S, Abrams RA, et al. Resected adenocarcinoma of the pancreas–616 patients: results, outcomes, and prognostic indicators. J Gastrointest Surg. 2000;4:567–579. - PubMed
-
- Connor S, Alexakis N, Garden OJ, Leandros E, Bramis J, Wigmore SJ. Meta-analysis of the value of somatostatin and its analogues in reducing complications associated with pancreatic surgery. Br J Surg. 2005;92:1059–1067. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
