

Hepatic resection for post-cholecystectomy bile duct injuries: a literature review
- PMID: 20590909
- PMCID: PMC2951822
- DOI: 10.1111/j.1477-2574.2010.00172.x
Hepatic resection for post-cholecystectomy bile duct injuries: a literature review
Abstract
Objectives: This study seeks to identify factors for hepatectomy in the management of post-cholecystectomy bile duct injury (BDI) and outcome via a systematic review of the literature.
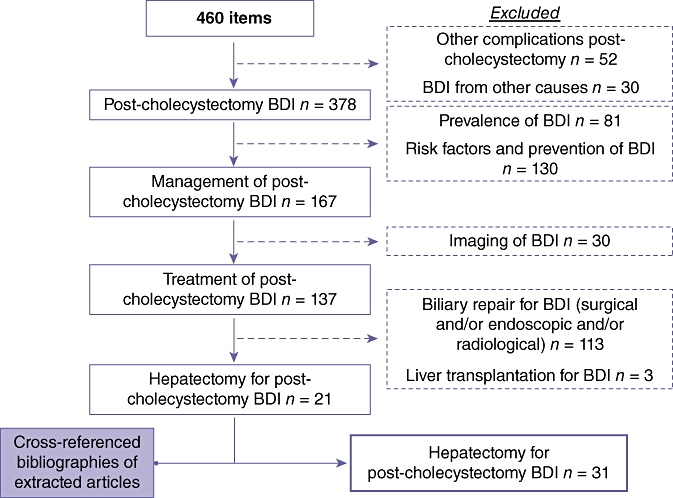
Methods: Relevant literature was found by searching the PubMed database and the bibliographies of extracted articles. To avoid bias selection, factors for hepatectomy were analysed in series reporting both patients undergoing hepatectomy and patients undergoing biliary repair without hepatectomy (bimodal treatment). Relevant variables were the presence or absence of additional hepatic artery and/or portal vein injury, the level of BDI, and a previous biliary repair.
Results: Among 460 potentially relevant publications, only 31 met the eligibility criteria. A total of 99 hepatectomies were reported among 1756 (5.6%) patients referred for post-cholecystectomy BDI. In eight series reporting bimodal treatment, including 232 patients, logistic regression multivariate analysis showed that hepatic arterial and Strasberg E4 and E5 injuries were independent factors associated with hepatectomy. Patients with combined arterial and Strasberg E4 or E5 injury were 43.3 times more likely to undergo hepatectomy (95% confidence interval 8.0-234.2) than patients without complex injury. Despite high postoperative morbidity, mortality rates were comparable with those of hepaticojejunostomy, except in urgent hepatectomies (within 2 weeks; four of nine patients died). Longterm outcome was satisfactory in 12 of 18 patients in the largest series.
Conclusions: Hepatectomies were performed mainly in patients showing complex concurrent Strasberg E4 or E5 and hepatic arterial injury and provided satisfactory longterm outcomes despite high postoperative morbidity.
Figures
Similar articles
-
Utility of fluorescent cholangiography during laparoscopic cholecystectomy: A systematic review.World J Gastroenterol. 2015 Jul 7;21(25):7877-83. doi: 10.3748/wjg.v21.i25.7877. World J Gastroenterol. 2015. PMID: 26167088 Free PMC article.
-
Hepatectomy after bile duct injury: a systematic review.HPB (Oxford). 2022 Feb;24(2):161-168. doi: 10.1016/j.hpb.2021.09.012. Epub 2021 Oct 5. HPB (Oxford). 2022. PMID: 34702627
-
Minimally invasive biliary anastomosis after iatrogenic bile duct injury: a systematic review.Updates Surg. 2023 Jan;75(1):31-39. doi: 10.1007/s13304-022-01392-5. Epub 2022 Oct 7. Updates Surg. 2023. PMID: 36205829
-
Single-incision laparoscopic cholecystectomy: does it work? A systematic review.Surg Endosc. 2016 Oct;30(10):4389-99. doi: 10.1007/s00464-016-4757-5. Epub 2016 Feb 19. Surg Endosc. 2016. PMID: 26895901
-
Bile Duct Injury: A Novel Risk Stratification System for the Timing of Repair.Am Surg. 2025 Jul;91(7):1163-1169. doi: 10.1177/00031348251332689. Epub 2025 Apr 3. Am Surg. 2025. PMID: 40179391
Cited by
-
Severe case of post cholecystectomy vasculobiliary injury successfully treated by right hepatectomy with a jump graft to the remaining left hepatic lobe.J Surg Case Rep. 2020 Sep 24;2020(9):rjaa319. doi: 10.1093/jscr/rjaa319. eCollection 2020 Sep. J Surg Case Rep. 2020. PMID: 33005319 Free PMC article.
-
Timing and risk factors of hepatectomy in the management of complications following laparoscopic cholecystectomy.J Gastrointest Surg. 2012 Apr;16(4):815-20. doi: 10.1007/s11605-011-1769-2. Epub 2011 Nov 9. J Gastrointest Surg. 2012. PMID: 22068969
-
Stepwise approach to curative surgery using percutaneous transhepatic cholangiodrainage and portal vein embolization for severe bile duct injury during laparoscopic cholecystectomy: a case report.Surg Case Rep. 2016 Dec;2(1):27. doi: 10.1186/s40792-016-0154-5. Epub 2016 Mar 17. Surg Case Rep. 2016. PMID: 26989053 Free PMC article.
-
Hepatectomy for bile duct injuries: when is it necessary?World J Gastroenterol. 2013 Oct 14;19(38):6348-52. doi: 10.3748/wjg.v19.i38.6348. World J Gastroenterol. 2013. PMID: 24151352 Free PMC article.
-
Four-Year Report of Iatrogenic Bile Duct Injury Repair from a Referral Hepatobiliary Center.Middle East J Dig Dis. 2024 Jul;16(3):173-177. doi: 10.34172/mejdd.2024.385. Epub 2024 Jul 31. Middle East J Dig Dis. 2024. PMID: 39386338 Free PMC article.
References
-
- Strasberg SM, Hertl M, Soper NJ. An analysis of the problem of biliary injury during laparoscopic cholecystectomy. J Am Coll Surg. 1995;180:101–125. - PubMed
-
- Schmidt SC, Langrehr JM, Hintze RE, Neuhaus P. Longterm results and risk factors influencing outcome of major bile duct injuries following cholecystectomy. Br J Surg. 2005;92:76–82. - PubMed
-
- Vitale GC, Tran TC, Davis BR, Vitale M, Vitale D, Larson G. Endoscopic management of post-cholecystectomy bile duct strictures. J Am Coll Surg. 2008;206:918–923. discussion 924–925. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
