

Comparison of actual surgical outcomes and 3-dimensional surgical simulations
- PMID: 20591553
- PMCID: PMC2945446
- DOI: 10.1016/j.joms.2009.09.058
Comparison of actual surgical outcomes and 3-dimensional surgical simulations
Abstract
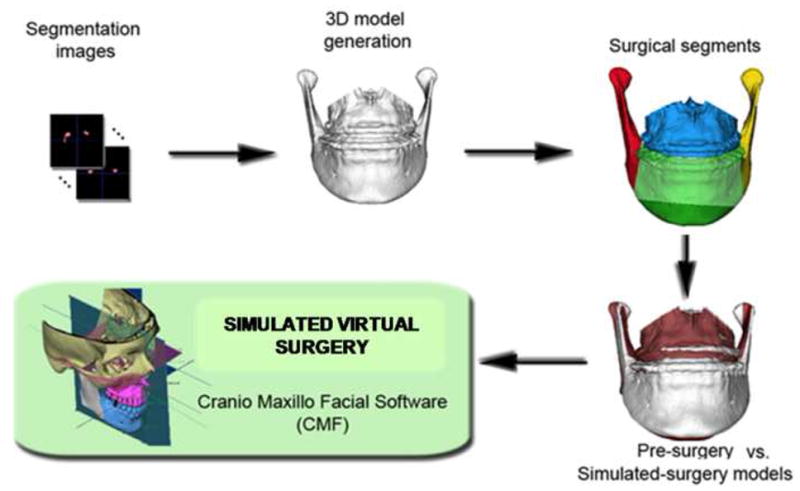
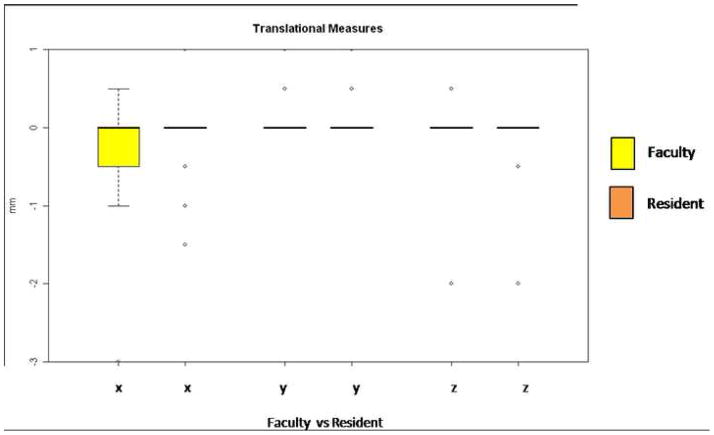
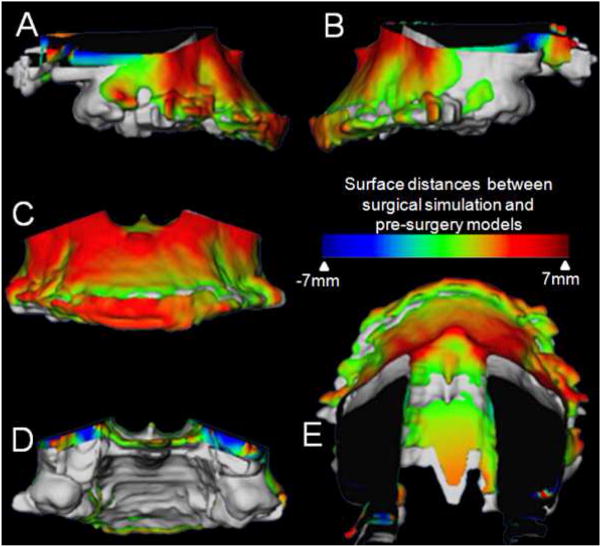
Purpose: The advent of imaging software programs has proved to be useful for diagnosis, treatment planning, and outcome measurement, but precision of 3-dimensional (3D) surgical simulation still needs to be tested. This study was conducted to determine whether the virtual surgery performed on 3D models constructed from cone-beam computed tomography (CBCT) can correctly simulate the actual surgical outcome and to validate the ability of this emerging technology to recreate the orthognathic surgery hard tissue movements in 3 translational and 3 rotational planes of space.
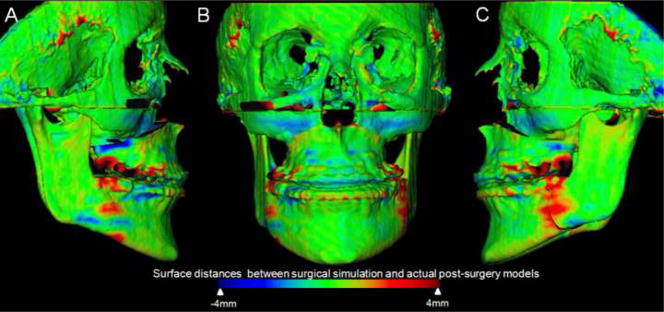
Materials and methods: Construction of pre- and postsurgery 3D models from CBCTs of 14 patients who had combined maxillary advancement and mandibular setback surgery and 6 patients who had 1-piece maxillary advancement surgery was performed. The postsurgery and virtually simulated surgery 3D models were registered at the cranial base to quantify differences between simulated and actual surgery models. Hotelling t tests were used to assess the differences between simulated and actual surgical outcomes.
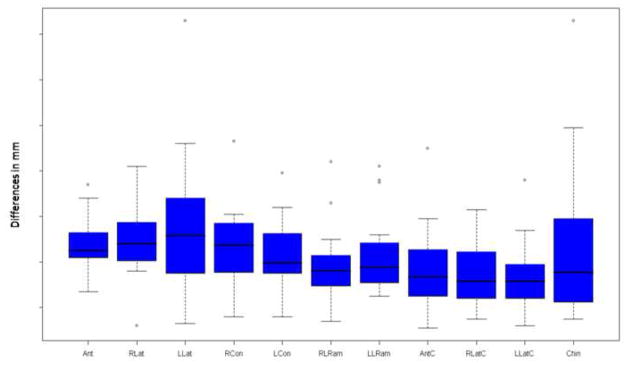
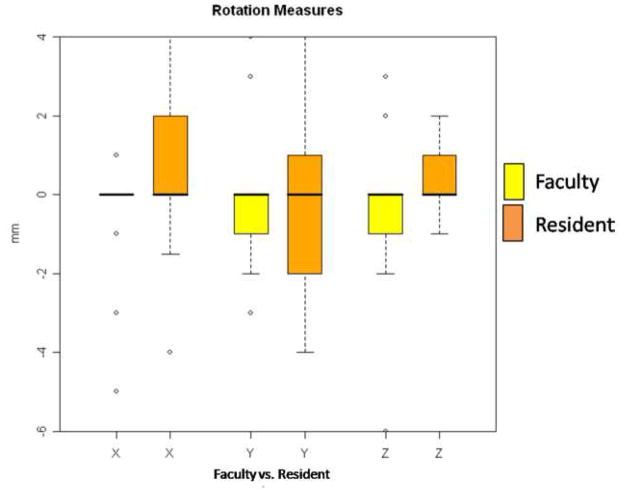
Results: For all anatomic regions of interest, there was no statistically significant difference between the simulated and the actual surgical models. The right lateral ramus was the only region that showed a statistically significant, but small difference when comparing 2- and 1-jaw surgeries.
Conclusions: Virtual surgical methods were reliably reproduced. Oral surgery residents could benefit from virtual surgical training. Computer simulation has the potential to increase predictability in the operating room.
Copyright © 2010 American Association of Oral and Maxillofacial Surgeons. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Loh S, Yow M. Computer prediction of hard tissue profiles in orthognathic surgery. Int J Adult Orthodon Orthognath Surg. 2002;17(4):342–7. - PubMed
-
- Loh S, Heng JK, Ward-Booth P, Winchester L, McDonald F. A radiographic analysis of computer prediction in conjunction with orthognathic surgery. Int J Oral Maxillofac Surg. 2001;30(4):259–63. - PubMed
-
- Mankad B, Cisneros GJ, Freeman K, Eisig SB. Prediction accuracy of soft tissue profile in orthognathic surgery. Int J Adult Orthodon Orthognath Surg. 1999;14(1):19–26. - PubMed
-
- Pektas ZO, Kircelli BH, Cilasun U, Uckan S. The accuracy of computer-assisted surgical planning in soft tissue prediction following orthognathic surgery. Int J Med Robot. 2007;3:64–71. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
