

From pre-diabetes to type 2 diabetes in obese youth: pathophysiological characteristics along the spectrum of glucose dysregulation
- PMID: 20592052
- PMCID: PMC2945164
- DOI: 10.2337/dc10-0004
From pre-diabetes to type 2 diabetes in obese youth: pathophysiological characteristics along the spectrum of glucose dysregulation
Abstract
Objective: Impaired fasting glucose (IFG) and impaired glucose tolerance (IGT) are considered pre-diabetes states. There are limited data in pediatrics in regard to their pathophysiology. We investigated differences in insulin sensitivity and secretion among youth with IFG, IGT, and coexistent IFG/IGT compared with those with normal glucose tolerance (NGT) and type 2 diabetes.
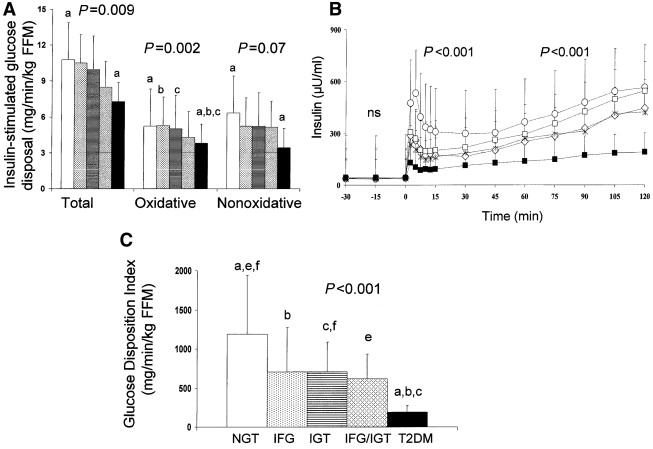
Research design and methods: A total of 24 obese adolescents with NGT, 13 with IFG, 29 with IGT, 11 with combined IFG/IGT, and 30 with type 2 diabetes underwent evaluation of hepatic glucose production ([6,6-(2)H(2)]glucose), insulin-stimulated glucose disposal (R(d), euglycemic clamp), first- and second-phase insulin secretion (hyperglycemic clamp), body composition (dual-energy X-ray absorptiometry), abdominal adiposity (computed tomography), and substrate oxidation (indirect calorimetry).
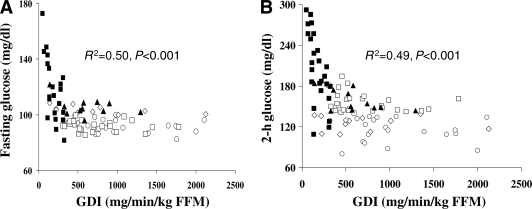
Results: Adolescents with NGT, pre-diabetes, and type 2 diabetes had similar body composition and abdominal fat distribution. R(d) was lower (P = 0.009) in adolescents with type 2 diabetes than in those with NGT. Compared with adolescents with NGT, first-phase insulin was lower in those with IFG, IGT, and IFG/IGT with further deterioration in those with type 2 diabetes (P < 0.001), and β-cell function relative to insulin sensitivity (glucose disposition index [GDI]) was also lower in those with IFG, IGT, and IFG/IGT (40, 47, and 47%, respectively), with a further decrease (80%) in those with type 2 diabetes (P < 0.001). GDI was the major determinant of fasting and 2-h glucose levels.
Conclusions: Obese adolescents who show signs of glucose dysregulation, including abnormal fasting glucose, glucose intolerance or both, are more likely to have impaired insulin secretion rather than reduced insulin sensitivity. Given the impairment in insulin secretion, they are at high risk for progression to type 2 diabetes. Further deterioration in insulin sensitivity or secretion may enhance the risk for this progression.
Figures
References
-
- American Diabetes Association Screening for type 2 diabetes. Diabetes Care 2004;27:(Suppl. 1)S11–S14 - PubMed
-
- Benjamin S, Cadwell B, Geiss L, Engelgau M, Vinicor F: A change in definition results in an increased number of adults with prediabetes in the United States. Arch Intern Med 2004;164:2386. - PubMed
-
- Williams DE, Cadwell BL, Cheng YJ, Cowie CC, Gregg EW, Geiss LS, Engelgau MM, Narayan KM, Imperatore G: Prevalence of impaired fasting glucose and its relationship with cardiovascular disease risk factors in US adolescents, 1999–2000. Pediatrics 2005;116:1122–1126 - PubMed
-
- Tripathy D, Carlsson M, Almgren P, Isomaa B, Taskinen MR, Tuomi T, Groop LC: Insulin secretion and insulin sensitivity in relation to glucose tolerance: lessons from the Botnia Study. Diabetes 2000;49:975–980 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
