

Contrast-enhanced MR imaging of lymph nodes in cancer patients
- PMID: 20592922
- PMCID: PMC2893309
- DOI: 10.3348/kjr.2010.11.4.383
Contrast-enhanced MR imaging of lymph nodes in cancer patients
Abstract
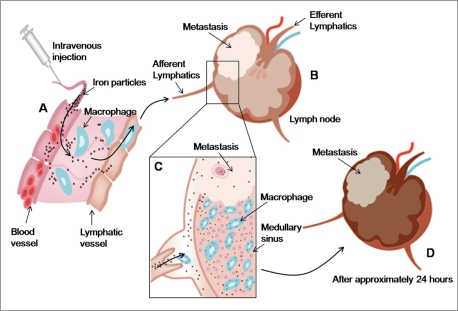
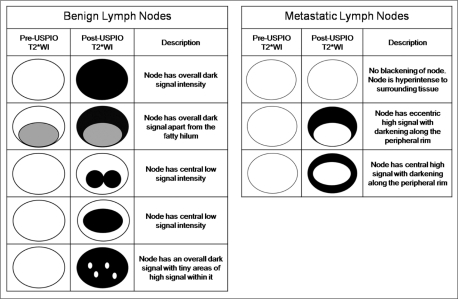
The accurate identification and characterization of lymph nodes by modern imaging modalities has important therapeutic and prognostic significance for patients with newly diagnosed cancers. The presence of nodal metastases limits the therapeutic options, and it generally indicates a worse prognosis for the patients with nodal metastases. Yet anatomic imaging (CT and MR imaging) is of limited value for depicting small metastatic deposits in normal-sized nodes, and nodal size is a poor criterion when there is no extracapsular extension or focal nodal necrosis to rely on for diagnosing nodal metastases. Thus, there is a need for functional methods that can be reliably used to identify small metastases. Contrast-enhanced MR imaging of lymph nodes is a non-invasive method for the analysis of the lymphatic system after the interstitial or intravenous administration of contrast media. Moreover, some lymphotrophic contrast media have been developed and used for detecting lymph node metastases, and this detection is independent of the nodal size. This article will review the basic principles, the imaging protocols, the interpretation and the accuracies of contrast-enhanced MR imaging of lymph nodes in patients with malignancies, and we also focus on the recent issues cited in the literature. In addition, we discuss the results of several pre-clinical studies and animal studies that were conducted in our institution.
Keywords: Contrast media; Lymph node metastasis; Magnetic resonance (MR); Magnetic resonance (MR) lymphography.
Figures
Similar articles
-
[Contrast media for magnetic resonance tomographic lymph node diagnosis (MR lymphography)].Radiologe. 1996 Feb;36(2):134-40. doi: 10.1007/s001170050050. Radiologe. 1996. PMID: 8867430 Review. German.
-
MR contrast agents in lymph node imaging.Eur J Radiol. 2006 Jun;58(3):375-82. doi: 10.1016/j.ejrad.2005.12.044. Epub 2006 Feb 7. Eur J Radiol. 2006. PMID: 16464554 Review.
-
Experimental lymph node metastases: enhanced detection with MR lymphography.Radiology. 1989 Jun;171(3):835-9. doi: 10.1148/radiology.171.3.2717761. Radiology. 1989. PMID: 2717761
-
Lymph node metastasis: ultrasmall superparamagnetic iron oxide-enhanced MR imaging versus PET/CT in a rabbit model.Radiology. 2007 Jan;242(1):137-43. doi: 10.1148/radiol.2421060093. Epub 2006 Nov 7. Radiology. 2007. PMID: 17090719
-
Prostate cancer: detection of lymph node metastases outside the routine surgical area with ferumoxtran-10-enhanced MR imaging.Radiology. 2009 May;251(2):408-14. doi: 10.1148/radiol.2512071018. Radiology. 2009. PMID: 19401573
Cited by
-
Effects of ferumoxytol on quantitative PET measurements in simultaneous PET/MR whole-body imaging: a pilot study in a baboon model.EJNMMI Phys. 2015 Dec;2(1):6. doi: 10.1186/s40658-015-0109-0. Epub 2015 Feb 26. EJNMMI Phys. 2015. PMID: 26501808 Free PMC article.
-
Fat-suppressed gadolinium-enhanced isotropic high-resolution 3D-GRE-T1WI for predicting small node metastases in patients with rectal cancer.Cancer Imaging. 2018 May 21;18(1):21. doi: 10.1186/s40644-018-0153-9. Cancer Imaging. 2018. PMID: 29784058 Free PMC article.
-
Predicting of axillary lymph node metastasis in invasive breast cancer using multiparametric MRI dataset based on CNN model.Front Oncol. 2022 Dec 6;12:1069733. doi: 10.3389/fonc.2022.1069733. eCollection 2022. Front Oncol. 2022. PMID: 36561533 Free PMC article.
-
The mechanical responses of advecting cells in confined flow.Biomicrofluidics. 2020 May 4;14(3):031501. doi: 10.1063/5.0005154. eCollection 2020 May. Biomicrofluidics. 2020. PMID: 32454924 Free PMC article. Review.
-
Comparison of Two Ultrasmall Superparamagnetic Iron Oxides on Cytotoxicity and MR Imaging of Tumors.Theranostics. 2012;2(1):76-85. doi: 10.7150/thno.3462. Epub 2012 Jan 1. Theranostics. 2012. PMID: 22272221 Free PMC article.
References
-
- King AD, Tse GM, Ahuja AT, Yuen EH, Vlantis AC, To EW, et al. Necrosis in metastatic neck nodes: diagnostic accuracy of CT, MR imaging, and US. Radiology. 2004;230:720–726. - PubMed
-
- Anzai Y, Brunberg JA, Lufkin RB. Imaging of nodal metastases in the head and neck. J Magn Reson Imaging. 1997;7:774–783. - PubMed
-
- Gershenwald JE, Thompson W, Mansfield PF, Lee JE, Colome MI, Tseng CH, et al. Multi-institutional melanoma lymphatic mapping experience: the prognostic value of sentinel lymph node status in 612 stage I or II melanoma patients. J Clin Oncol. 1999;17:976–983. - PubMed
-
- Laissy JP, Gay-Depassier P, Soyer P, Dombret MC, Murciano G, Sautet A, et al. Enlarged mediastinal lymph nodes in bronchogenic carcinoma: assessment with dynamic contrast-enhanced MR imaging. Work in progress. Radiology. 1994;191:263–267. - PubMed
-
- van den Brekel MW. Lymph node metastases: CT and MRI. Eur J Radiol. 2000;33:230–238. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
