

Malignant colorectal polyps
- PMID: 20593495
- PMCID: PMC2896747
- DOI: 10.3748/wjg.v16.i25.3103
Malignant colorectal polyps
Abstract
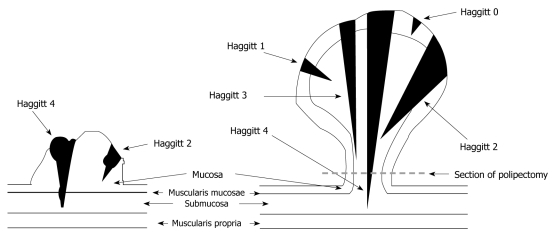
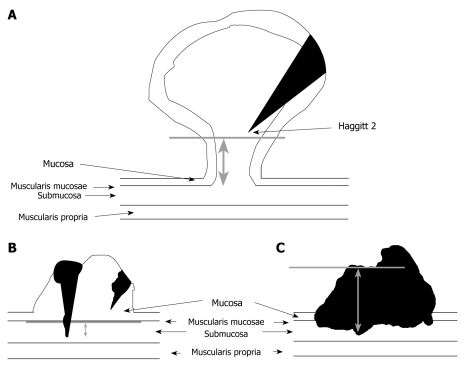
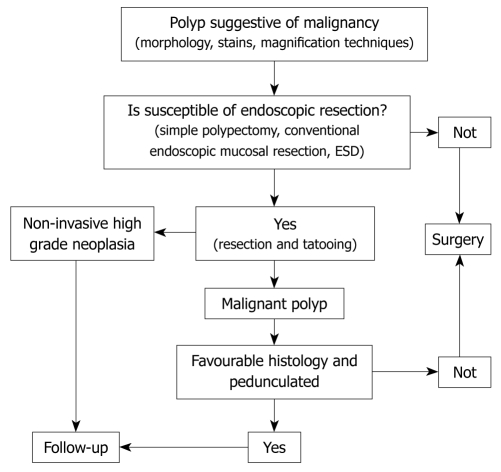
Nowadays, the number of cases in which malignant colorectal polyps are removed is increasing due to colorectal cancer screening programmes. Cancerous polyps are classified into non-invasive high grade neoplasia (NHGN), when the cancer has not reached the muscularis mucosa, and malignant polyps, classed as T1, when they have invaded the submucosa. NHGN is considered cured with polypectomy, while the prognosis for malignant polyps depends on various morphological and histological factors. The prognostic factors include, sessile or pedunculated morphology of the polyp, whether partial or en bloc resection is carried out, the degree of differentiation of the carcinoma, vascular or lymphatic involvement, and whether the polypectomy resection margin is tumor free. A malignant polyp at T1 is considered cured with polypectomy if it is a pedunculated polyp (Ip of the Paris classification), it has been completely resected, it is not poorly differentiated, the resection edge is not affected by the tumor and there is no vascular or lymphatic involvement. The sessile malignant polyp (Is of the Paris classification) at T1 is considered not cured with polypectomy. Only in some cases (e.g. older people with high surgical risk) local excision (polypectomy or endoscopic submucosal dissection or conventional endoscopic mucosal resection) is considered the definitive treatment.
Figures
References
-
- Castells A, Marzo-Castillejo M, Mascort JJ, Amador FJ, Andreu M, Bellas B, Ferrandez A, Ferrandiz J, Giraldez M, Gonzalo V, Jover R, Quintero E, Alonso-Coello P, Bonfill X, Lanas A, Pinol V, Pique J. [In process citation] Gastroenterol Hepatol. 2009;32:717.e1–717.e58. - PubMed
-
- Piñol V, Andreu M, Castells A, Payá A, Bessa X, Rodrigo J. Frequency of hereditary non-polyposis colorectal cancer and other colorectal cancer familial forms in Spain: a multicentre, prospective, nationwide study. Eur J Gastroenterol Hepatol. 2004;16:39–45. - PubMed
-
- Volk EE, Goldblum JR, Petras RE, Carey WD, Fazio VW. Management and outcome of patients with invasive carcinoma arising in colorectal polyps. Gastroenterology. 1995;109:1801–1807. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
