

Absence of evidence of xenotropic murine leukemia virus-related virus infection in persons with chronic fatigue syndrome and healthy controls in the United States
- PMID: 20594299
- PMCID: PMC2908559
- DOI: 10.1186/1742-4690-7-57
Absence of evidence of xenotropic murine leukemia virus-related virus infection in persons with chronic fatigue syndrome and healthy controls in the United States
Abstract
Background: XMRV, a xenotropic murine leukemia virus (MuLV)-related virus, was recently identified by PCR testing in 67% of persons with chronic fatigue syndrome (CFS) and in 3.7% of healthy persons from the United States. To investigate the association of XMRV with CFS we tested blood specimens from 51 persons with CFS and 56 healthy persons from the US for evidence of XMRV infection by using serologic and molecular assays. Blinded PCR and serologic testing were performed at the US Centers for Disease Control and Prevention (CDC) and at two additional laboratories.
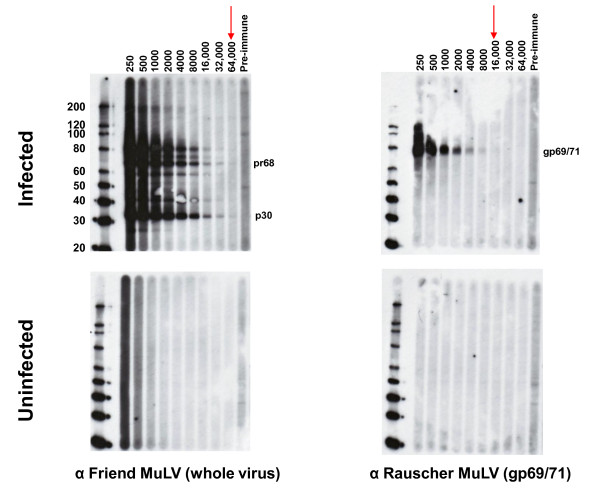
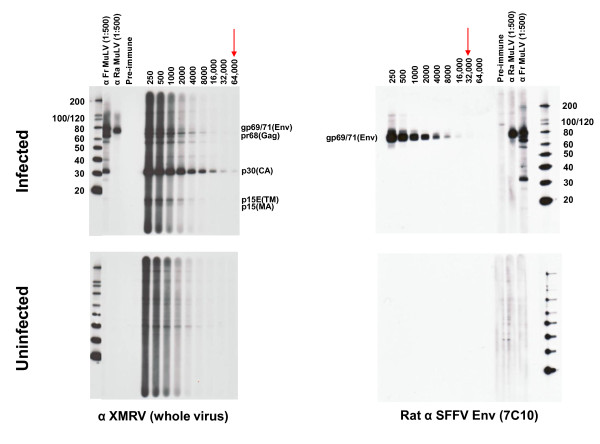
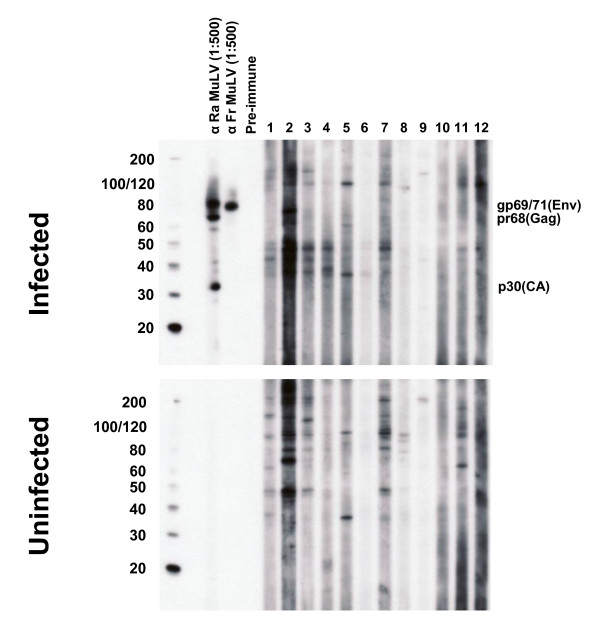
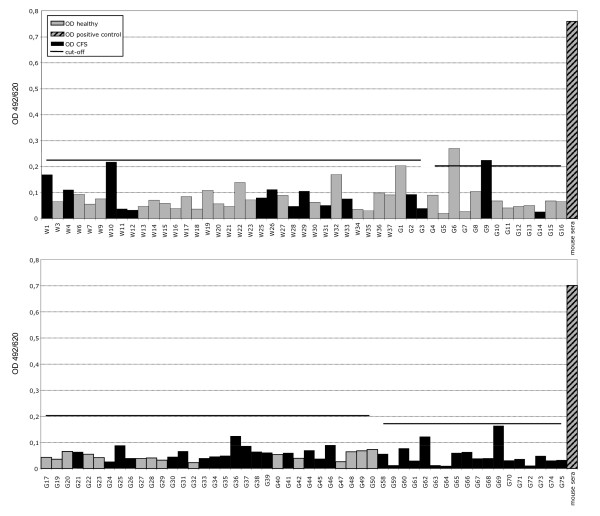
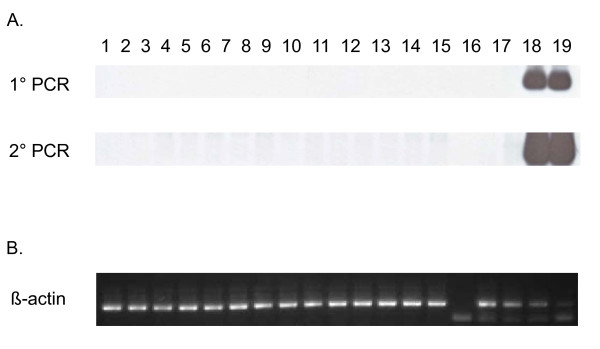
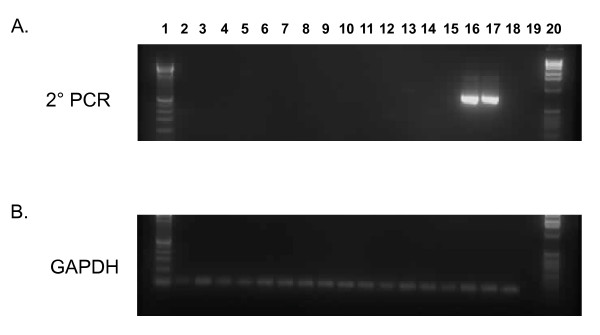
Results: Archived blood specimens were tested from persons with CFS defined by the 1994 international research case definition and matched healthy controls from Wichita, Kansas and metropolitan, urban, and rural Georgia populations. Serologic testing at CDC utilized a Western blot (WB) assay that showed excellent sensitivity to MuLV and XMRV polyclonal or monoclonal antibodies, and no reactivity on sera from 121 US blood donors or 26 HTLV-and HIV-infected sera. Plasma from 51 CFS cases and plasma from 53 controls were all WB negative. Additional blinded screening of the 51 cases and 53 controls at the Robert Koch Institute using an ELISA employing recombinant Gag and Env XMRV proteins identified weak seroreactivity in one CFS case and a healthy control, which was not confirmed by immunofluorescence. PCR testing at CDC employed a gag and a pol nested PCR assay with a detection threshold of 10 copies in 1 ug of human DNA. DNA specimens from 50 CFS patients and 56 controls and 41 US blood donors were all PCR-negative. Blinded testing by a second nested gag PCR assay at the Blood Systems Research Institute was also negative for DNA specimens from the 50 CFS cases and 56 controls.
Conclusions: We did not find any evidence of infection with XMRV in our U.S. study population of CFS patients or healthy controls by using multiple molecular and serologic assays. These data do not support an association of XMRV with CFS.
Figures
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
