

Increased duration of mechanical ventilation is associated with decreased diaphragmatic force: a prospective observational study
- PMID: 20594319
- PMCID: PMC2945090
- DOI: 10.1186/cc9094
Increased duration of mechanical ventilation is associated with decreased diaphragmatic force: a prospective observational study
Abstract
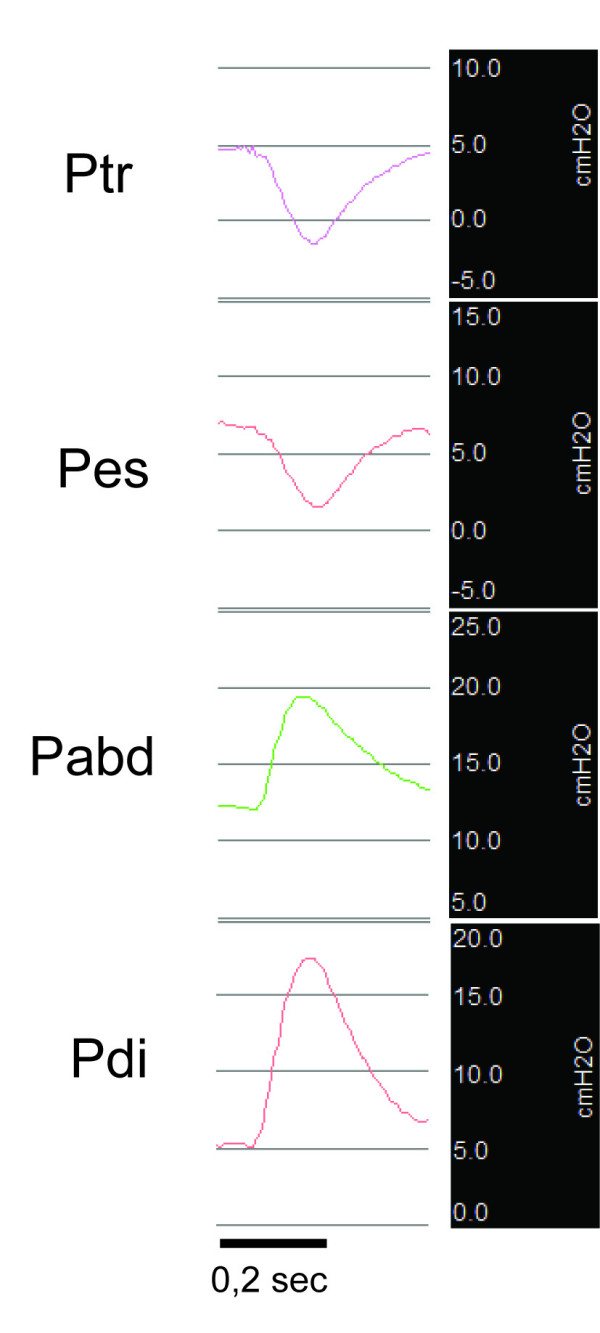
Introduction: Respiratory muscle weakness is an important risk factor for delayed weaning. Animal data show that mechanical ventilation itself can cause atrophy and weakness of the diaphragm, called ventilator-induced diaphragmatic dysfunction (VIDD). Transdiaphragmatic pressure after magnetic stimulation (TwPdi BAMPS) allows evaluation of diaphragm strength. We aimed to evaluate the repeatability of TwPdi BAMPS in critically ill, mechanically ventilated patients and to describe the relation between TwPdi and the duration of mechanical ventilation.
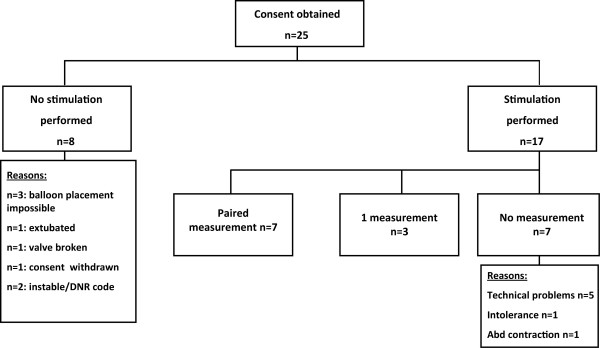
Methods: This was a prospective observational study in critically ill and mechanically ventilated patients, admitted to the medical intensive care unit of a university hospital. Nineteen measurements were made in a total of 10 patients at various intervals after starting mechanical ventilation. In seven patients, measurements were made on two or more occasions, with a minimum interval of 24 hours.
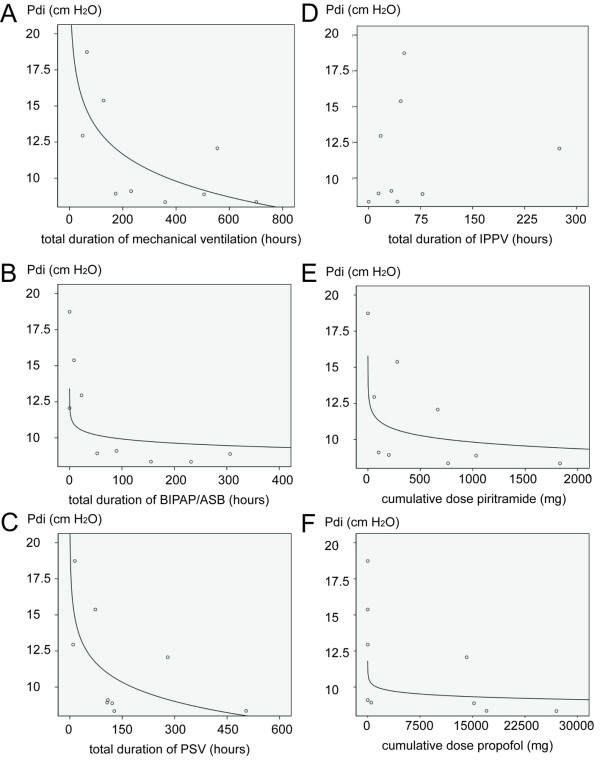
Results: The TwPdi was 11.5 ± 3.9 cm H2O (mean ± SD), indicating severe respiratory muscle weakness. The between-occasion coefficient of variation of TwPdi was 9.7%, comparable with data from healthy volunteers. Increasing duration of mechanical ventilation was associated with a logarithmic decline in TwPdi (R = 0.69; P = 0.038). This association was also found for cumulative time on pressure control (R = 0.71; P = 0.03) and pressure-support ventilation (P = 0.05; R = 0.66) separately, as well as for cumulative dose of propofol (R = 0.66; P = 0.05) and piritramide (R = 0.79; P = 0.01).
Conclusions: Duration of mechanical ventilation is associated with a logarithmic decline in diaphragmatic force, which is compatible with the concept of VIDD. The observed decline may also be due to other potentially contributing factors such as sedatives/analgesics, sepsis, or others.
Figures
Comment in
-
Diaphragm weakness and mechanical ventilation--what's the critical issue?Crit Care. 2010;14(4):187. doi: 10.1186/cc9189. Epub 2010 Aug 4. Crit Care. 2010. PMID: 20701738 Free PMC article.
References
-
- Esteban A, Anzueto A, Frutos F, Alia I, Brochard L, Stewart TE, Benito S, Epstein SK, Apezteguia C, Nightingale P, Arroliga AC, Tobin MJ. Characteristics and outcomes in adult patients receiving mechanical ventilation: a 28-day international study. JAMA. 2002;287:345–355. doi: 10.1001/jama.287.3.345. - DOI - PubMed
-
- De Jonghe B, Sharshar T, Lefaucheur JP, Authier FJ, Durand-Zaleski I, Boussarsar M, Cerf C, Renaud E, Mesrati F, Carlet J, Raphael JC, Outin H, Bastuji-Garin S. Paresis acquired in the intensive care unit: a prospective multicenter study. JAMA. 2002;288:2859–2867. doi: 10.1001/jama.288.22.2859. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
