

Improving the evidence base of Markov models used to estimate the costs of scaling up antiretroviral programmes in resource-limited settings
- PMID: 20594369
- PMCID: PMC2895747
- DOI: 10.1186/1472-6963-10-S1-S3
Improving the evidence base of Markov models used to estimate the costs of scaling up antiretroviral programmes in resource-limited settings
Abstract
Background: Despite concerns about affordability and sustainability, many models of the lifetime costs of antiretroviral therapy (ART) used in resource limited settings are based on data from small research cohorts, together with pragmatic assumptions about life-expectancy. This paper revisits these modelling assumptions in order to provide input to future attempts to model the lifetime costs and the costs of scaling up ART.
Methods: We analysed the determinants of costs and outcomes in patients receiving ART in line with standard World Health Organization (WHO) guidelines for resource poor settings in a private sector managed ART programme in South Africa. The cohort included over 5,000 patients with up to 4 years (median 19 months) on ART. Generalized linear and Cox proportional hazards regression models were used to establish cost and outcome determinants respectively.
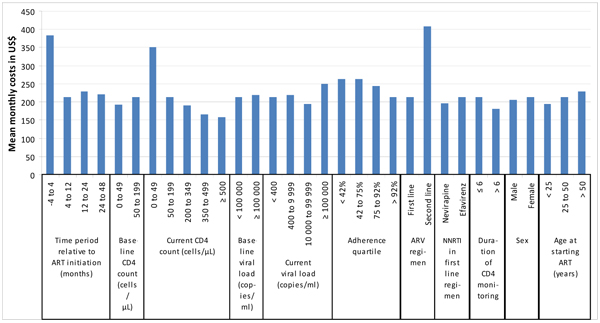
Results: The key variables associated with changes in mean monthly costs were: being on the second line regimen; receiving ART from 4 months prior to 4 months post treatment initiation; having a recent or current CD4 count <50 cells/microL or 50-199 cells/microl; having mean ART adherence <75% as determined by monthly pharmacy refill data; and having a current or recent viral load >100,000 copies/mL. In terms of the likelihood of dying, the key variables were: baseline CD4 count<50 cells/microl (particularly during the first 4 months on treatment); current CD4 count <50 cells/microl and 50-199 cells/microl (particularly during later periods on treatment); and being on the second line regimen. Being poorly adherent and having an unsuppressed viral load was also associated with a higher likelihood of dying.
Conclusions: While there are many unknowns associated with modelling the resources needed to scale-up ART, our analysis has suggested a number of key variables which can be used to improve the state of the art of modelling ART. While the magnitude of the effects associated with these variables would be likely to differ in other settings, the variables influencing costs and survival are likely to be generalizable. This is of direct relevance to those concerned about assessing the long-term costs and sustainability of expanded access to ART.
Figures
Similar articles
-
Early and late direct costs in a Southern African antiretroviral treatment programme: a retrospective cohort analysis.PLoS Med. 2009 Dec;6(12):e1000189. doi: 10.1371/journal.pmed.1000189. Epub 2009 Dec 1. PLoS Med. 2009. PMID: 19956658 Free PMC article.
-
Cost-effectiveness of HIV treatment in resource-poor settings--the case of Côte d'Ivoire.N Engl J Med. 2006 Sep 14;355(11):1141-53. doi: 10.1056/NEJMsa060247. N Engl J Med. 2006. PMID: 16971720
-
SESOTHO trial ("Switch Either near Suppression Or THOusand") - switch to second-line versus WHO-guided standard of care for unsuppressed patients on first-line ART with viremia below 1000 copies/mL: protocol of a multicenter, parallel-group, open-label, randomized clinical trial in Lesotho, Southern Africa.BMC Infect Dis. 2018 Feb 12;18(1):76. doi: 10.1186/s12879-018-2979-y. BMC Infect Dis. 2018. PMID: 29433430 Free PMC article. Clinical Trial.
-
The lifetime cost of current human immunodeficiency virus care in the United States.Med Care. 2006 Nov;44(11):990-7. doi: 10.1097/01.mlr.0000228021.89490.2a. Med Care. 2006. PMID: 17063130 Review.
-
Cost-Effectiveness of antiretroviral therapy: A systematic review.Indian J Public Health. 2020 Apr;64(Supplement):S32-S38. doi: 10.4103/ijph.IJPH_90_20. Indian J Public Health. 2020. PMID: 32295954
Cited by
-
Scaling up health policies and services in low- and middle-income settings.BMC Health Serv Res. 2010 Jul 2;10 Suppl 1(Suppl 1):I1. doi: 10.1186/1472-6963-10-S1-I1. BMC Health Serv Res. 2010. PMID: 20594366 Free PMC article.
-
A novel Markov model projecting costs and outcomes of providing antiretroviral therapy to public patients in private practices versus public clinics in South Africa.PLoS One. 2013;8(2):e53570. doi: 10.1371/journal.pone.0053570. Epub 2013 Feb 6. PLoS One. 2013. PMID: 23405073 Free PMC article.
-
Factors influencing retention in care after starting antiretroviral therapy in a rural South African programme.PLoS One. 2011 May 3;6(5):e19201. doi: 10.1371/journal.pone.0019201. PLoS One. 2011. PMID: 21559280 Free PMC article.
References
-
- WHO. Antiretroviral therapy for HIV infection in adults and adolescents in resource-limited settings: towards universal access: guidelines for a public health approach. Geneva: World Health Organization. 2006.
-
- Cleary S, Mooney G, McIntyre D. Equity and efficiency in HIV-treatment in South Africa: the contribution of mathematical programming to priority setting. Health Econ. 2009. DOI: 10.1002/hec.1542. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
