

Management of paragangliomas. Clinical and angiographic aspects
- PMID: 20594521
- PMCID: PMC3576606
- DOI: 10.1177/159101990200800204
Management of paragangliomas. Clinical and angiographic aspects
Abstract
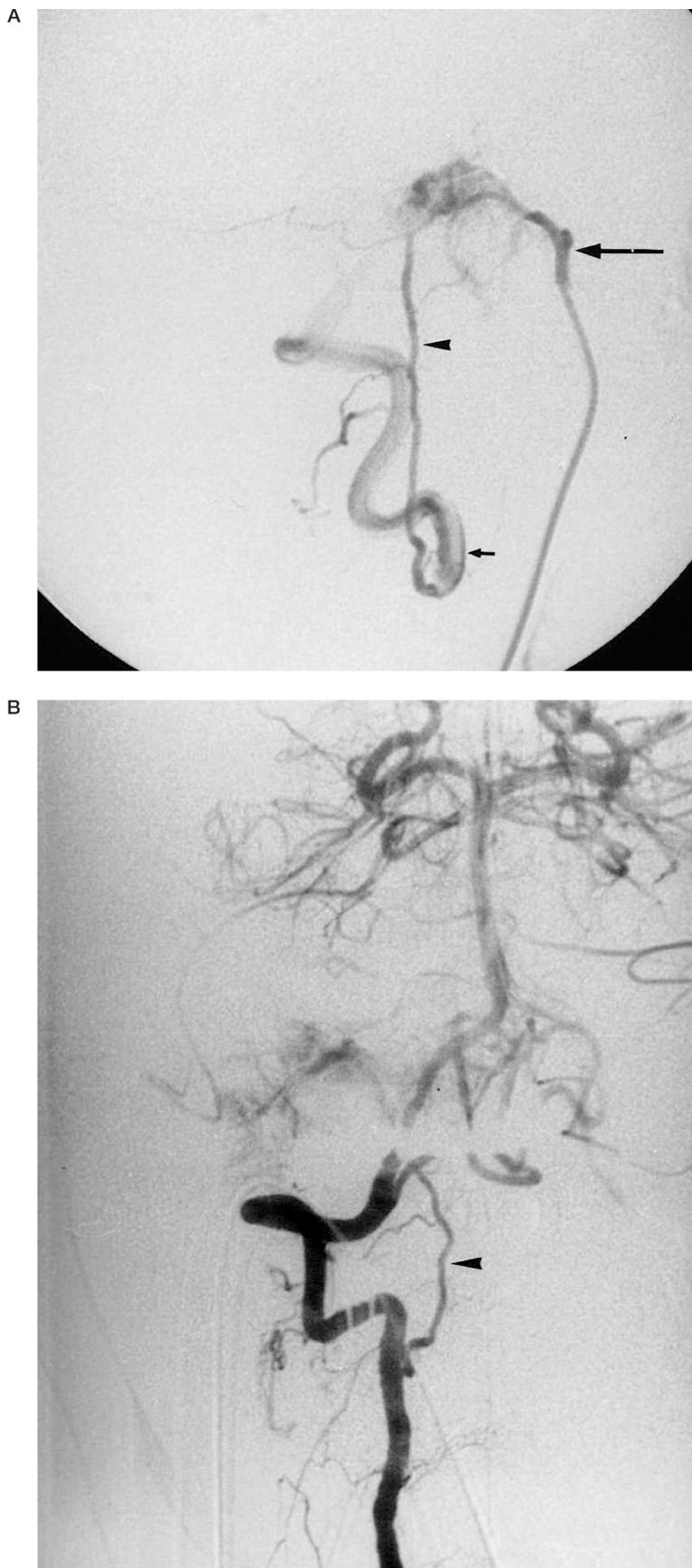
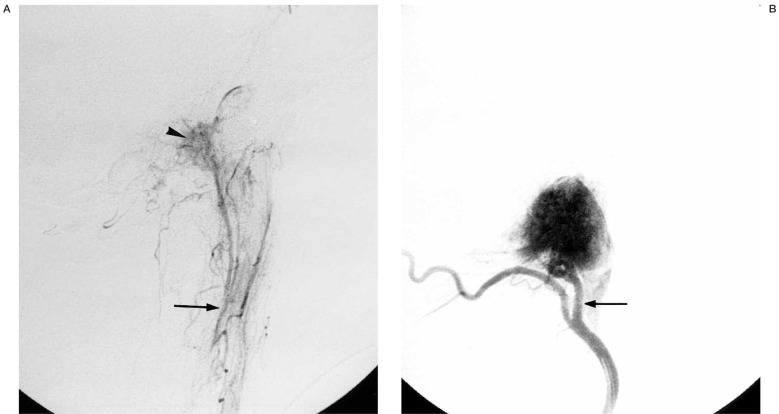
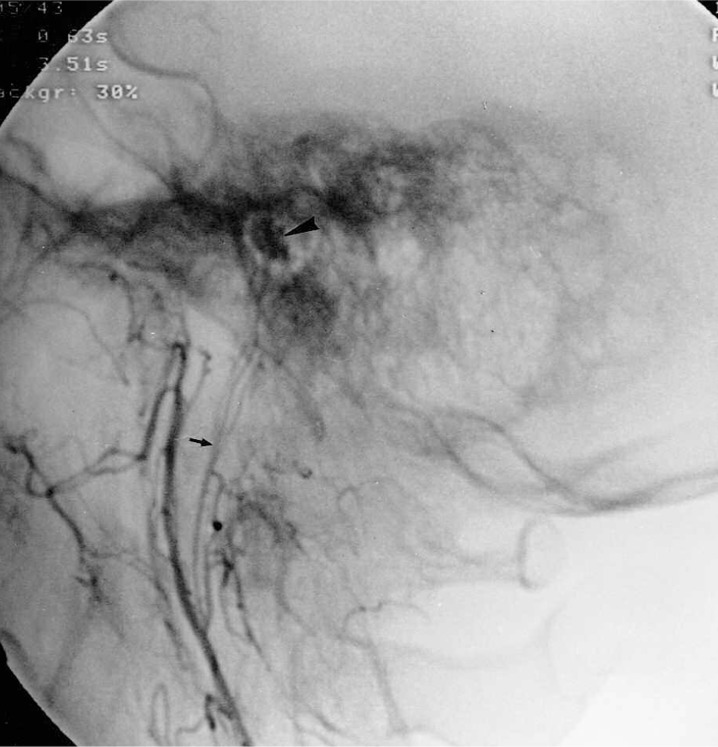
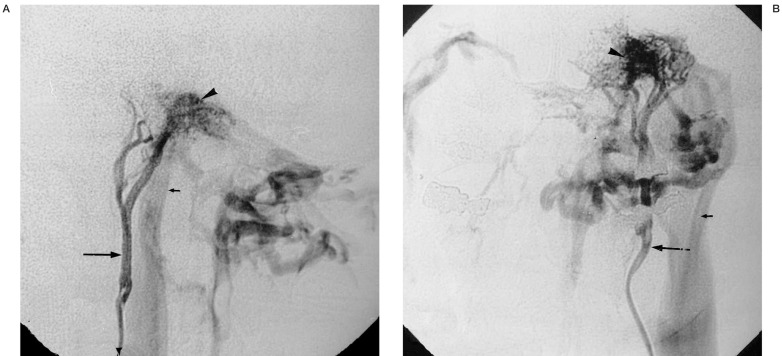
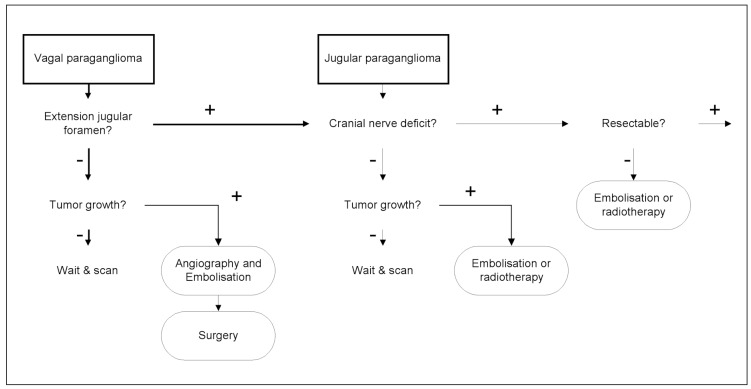
Head and neck paragangliomas are highly vascular tumors with variable clinical behavior. The goal of this paper is to determine specific clinical and radiological findings and extract from these findings a treatment algorithm. Twenty-three patients with paragangliomas were referred from different surgical centers for angiography and pre-operative embolization. Clinical records were analyzed retrospectively, and focused on impairment of cranial nerves. Angiographic features of paragangliomas, such as arterial supply, tumor flow characteristics, and venous drainage, were evaluated to find characteristic angioarchitectural patterns. All but one patient presented with a single tumor. All eight jugular and four of five vagal paragangliomas caused a lower cranial nerve deficit. Tympanic paragangliomas presented with hearing loss and tinnitus. The ascending pharyngeal artery was the main feeder and contributed to the supply in every tumor. Jugular and vagal paragangliomas typically compromise the patency of the jugular vein with resulting antegrade or retrograde flow through collateral venous systems. Surgical resection of vagal and jugular paragangliomas was especially performed when unifocal paragangliomas were present. In all of these patients, the tumor caused a cranial nerve deficit. The supply from an enlarged ascending pharyngeal artery is typical for paragangliomas. The venous drainage pattern of jugular and vagal paragangliomas allows differentiation from other vascular lesions at the skull base.
Figures
References
-
- Green D, Brackmann DE, et al. Surgical management of previously untreated glomus jugulare tumors. Laryngoscope. 1994;104:917–921. - PubMed
-
- Netterville JL, Jackson CG, et al. Vagal paraganglioma. Arch Otolaryngol Head Neck Surg. 1998;124:1133–1140. - PubMed
-
- O’Leary MJ, Shelton C, et al. Glomus tympanicum tumors: a clinical perspective. Laryngoscope. 1991;101:1038–1043. - PubMed
-
- Sillars HA, Fagan PA. The management of multiple paraganglioma of the head and neck. J Laryngol Otol. 1993;107:538–542. - PubMed
-
- Jackson CG. Neurotologic skull base surgery for glomus tumors. Diagnosis for treatment planning and treatment options. Laryngoscope. 1993;103:17–22. - PubMed
LinkOut - more resources
Full Text Sources
