

Preliminary evaluation of factors associated with premature trial closure and feasibility of accrual benchmarks in phase III oncology trials
- PMID: 20595245
- PMCID: PMC3977321
- DOI: 10.1177/1740774510374973
Preliminary evaluation of factors associated with premature trial closure and feasibility of accrual benchmarks in phase III oncology trials
Abstract
Background: A major challenge for randomized phase III oncology trials is the frequent low rates of patient enrollment, resulting in high rates of premature closure due to insufficient accrual.
Purpose: We conducted a pilot study to determine the extent of trial closure due to poor accrual, feasibility of identifying trial factors associated with sufficient accrual, impact of redesign strategies on trial accrual, and accrual benchmarks designating high failure risk in the clinical trials cooperative group (CTCG) setting.
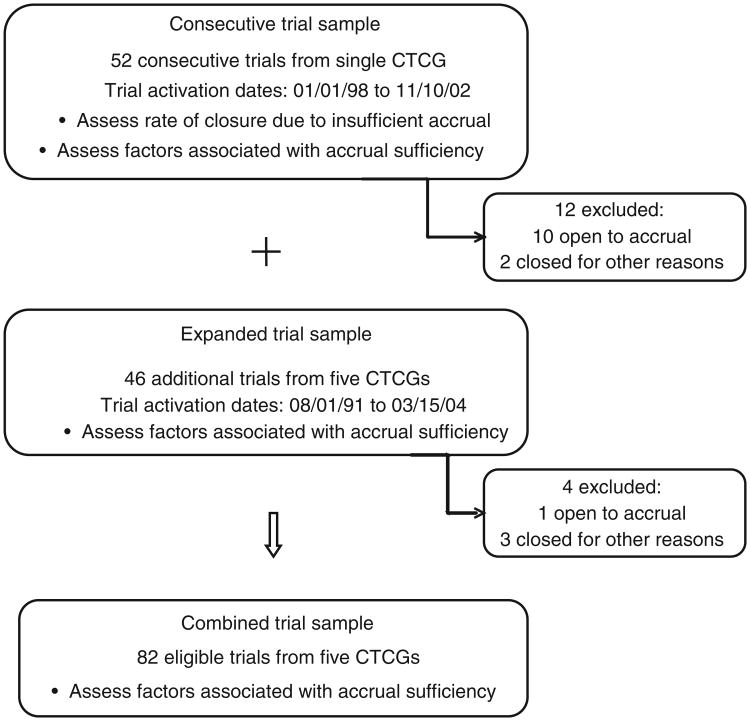
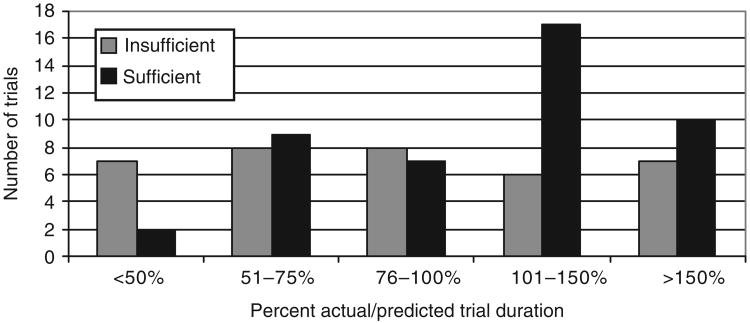
Methods: A subset of phase III trials opened by five CTCGs between August 1991 and March 2004 was evaluated. Design elements, experimental agents, redesign strategies, and pretrial accrual assessment supporting accrual predictions were abstracted from CTCG documents. Percent actual/predicted accrual rate averaged per month was calculated. Trials were categorized as having sufficient or insufficient accrual based on reason for trial termination. Analyses included univariate and bivariate summaries to identify potential trial factors associated with accrual sufficiency.
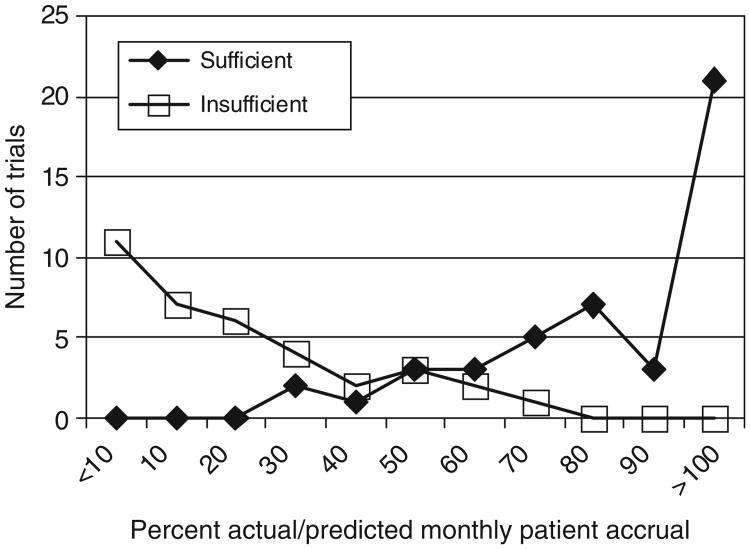
Results: Among 40 trials from one CTCG, 21 (52.5%) trials closed due to insufficient accrual. In 82 trials from five CTCGs, therapeutic trials accrued sufficiently more often than nontherapeutic trials (59% vs 27%, p = 0.05). Trials including pretrial accrual assessment more often achieved sufficient accrual than those without (67% vs 47%, p = 0.08). Fewer exclusion criteria, shorter consent forms, other CTCG participation, and trial design simplicity were not associated with achieving sufficient accrual. Trials accruing at a rate much lower than predicted (<35% actual/predicted accrual rate) were consistently closed due to insufficient accrual.
Limitations: This trial subset under-represents certain experimental modalities. Data sources do not allow accounting for all factors potentially related to accrual success.
Conclusion: Trial closure due to insufficient accrual is common. Certain trial design factors appear associated with attaining sufficient accrual. Defining accrual benchmarks for early trial termination or redesign is feasible, but better accrual prediction methods are critically needed. Future studies should focus on identifying trial factors that allow more accurate accrual predictions and strategies that can salvage open trials experiencing slow accrual.
Figures
References
-
- Lara PN, Jr, Higdon R, Lim N, et al. Prospective evaluation of cancer clinical trial accrual patterns: identifying potential barriers to enrollment. J Clin Oncol. 2001;19:1728–33. - PubMed
-
- Cassileth BR. Clinical trials: time for action. J Clin Oncol. 2003;21:765–66. - PubMed
-
- Prescott RJ, Counsell CE, Gillespie WJ, et al. Factors that limit the quality, number and progress of randomized controlled trials. Health Technol Assess. 1999;3:1–143. - PubMed
-
- Grunfeld E, Zitzelsberger L, Coristine M, Aspelund F. Barriers and facilitators to enrollment in cancer clinical trials: qualitative study of the perspectives of clinical research associates. Cancer. 2002;95:1577–83. - PubMed
-
- Ross S, Grant A, Counsell C, et al. Barriers to participation in randomized controlled trials: a systematic review. J Clin Epidemiol. 1999;52:1143–56. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
