

Use of an automated clinical management system improves outpatient immunosuppressive care following liver transplantation
- PMID: 20595306
- PMCID: PMC2995663
- DOI: 10.1136/jamia.2009.000992
Use of an automated clinical management system improves outpatient immunosuppressive care following liver transplantation
Abstract
Objective: Immunosuppressive therapy following transplantation, if not managed well, can lead to increased drug toxicity or rejection episodes. We investigated whether use of an automated clinical management system in our liver transplant program would improve clinical outcomes in managing transplant recipients' immunosuppressive medications.
Design: We performed a retrospective cohort study of two patient groups receiving liver transplants at our institution. One group of 301 patients transplanted from January 1, 2004 to November 30, 2006 received outpatient immunosuppressive management using a paper charting system. After instituting an automated clinical management system, the following group of 127 patients transplanted from December 12, 2006 to April 1, 2008 received their outpatient immunosuppressive management with that system. Only patients who received tacrolimus therapy, with or without mycophenolate mofetil or prednisone, were studied.
Measurements: Our endpoints included percentage of patients having rejection and/or tacrolimus toxicity episodes. Various recipient, intraoperative, donor, and postoperative variables, including managing the immunosuppressive therapy with a paper charting system or an automated management system, were studied to determine which factors were associated with our endpoints.
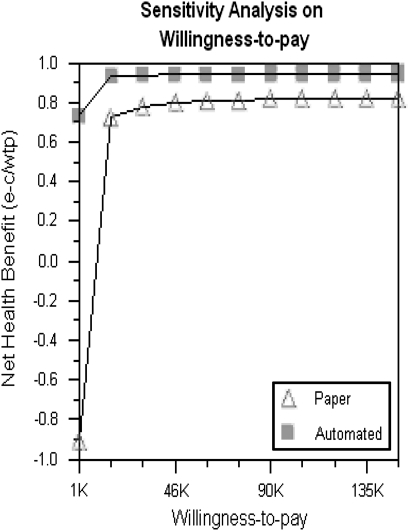
Results: Multivariable logistic regression analysis showed the automated system was significantly associated with fewer rejection episodes and fewer tacrolimus toxicity events. Formal cost-effectiveness analysis of the nurses' salaries for 1 year showed the automated system cost US$197 per patient and the paper system cost US$1703 per patient. The automated system improved quality of life years.
Conclusion: Use of an automated clinical management system for outpatient immunosuppressive management for liver transplant patients has resulted in a decrease in both tacrolimus toxicity and rejection episodes and is cost-effective.
Conflict of interest statement
Figures
Similar articles
-
Tacrolimus in pancreas transplantation: a multicenter analysis. Tacrolimus Pancreas Transplant Study Group.Clin Transplant. 1997 Aug;11(4):299-312. Clin Transplant. 1997. PMID: 9267719 Clinical Trial.
-
Mycophenolate mofetil in pancreas transplantation.Transplantation. 1998 Aug 15;66(3):318-23. doi: 10.1097/00007890-199808150-00007. Transplantation. 1998. PMID: 9721799
-
High tacrolimus intra-patient variability is associated with graft rejection, and de novo donor-specific antibodies occurrence after liver transplantation.World J Gastroenterol. 2018 Apr 28;24(16):1795-1802. doi: 10.3748/wjg.v24.i16.1795. World J Gastroenterol. 2018. PMID: 29713132 Free PMC article.
-
Tacrolimus: a further update of its use in the management of organ transplantation.Drugs. 2003;63(12):1247-97. doi: 10.2165/00003495-200363120-00006. Drugs. 2003. PMID: 12790696 Review.
-
Treatment strategies in pediatric solid organ transplant recipients with calcineurin inhibitor-induced nephrotoxicity.Pediatr Transplant. 2006 Sep;10(6):721-9. doi: 10.1111/j.1399-3046.2006.00577.x. Pediatr Transplant. 2006. PMID: 16911497 Review.
Cited by
-
Assessment of readiness for clinical decision support to aid laboratory monitoring of immunosuppressive care at U.S. liver transplant centers.Appl Clin Inform. 2014 Dec 17;5(4):988-1004. doi: 10.4338/ACI-2014-08-RA-0060. eCollection 2014. Appl Clin Inform. 2014. PMID: 25589912 Free PMC article.
-
Translation of evidence into kidney transplant clinical practice: managing drug-lab interactions by a context-aware clinical decision support system.BMC Med Inform Decis Mak. 2020 Aug 20;20(1):196. doi: 10.1186/s12911-020-01196-w. BMC Med Inform Decis Mak. 2020. PMID: 32819359 Free PMC article.
-
Telemedicine based remote monitoring after liver transplantation: Feasible in a select group and a more stringent control of immunosuppression.Clin Transplant. 2022 Jan;36(1):e14494. doi: 10.1111/ctr.14494. Epub 2021 Oct 1. Clin Transplant. 2022. PMID: 34596918 Free PMC article.
-
Adherence to immunosuppressive therapy following liver transplantation: an integrative review.Rev Lat Am Enfermagem. 2016 Aug 29;24:e2778. doi: 10.1590/1518-8345.1072.2778. Rev Lat Am Enfermagem. 2016. PMID: 27579933 Free PMC article. Review.
-
Longitudinal Analysis of Computerized Alerts for Laboratory Monitoring of Post-liver Transplant Immunosuppressive Care.AMIA Annu Symp Proc. 2015 Nov 5;2015:1918-26. eCollection 2015. AMIA Annu Symp Proc. 2015. PMID: 26958291 Free PMC article.
References
-
- Perkins JD, Levy AE, Duncan JB, et al. Using root cause analysis to improve survival in a liver transplant population. J Surg Res 2005;129:6–16 - PubMed
-
- Moench C, Barreiros AP, Schuchmann M, et al. Tacrolimus monotherapy without steroids after liver transplantation – a prospective randomized double-blinded placebo-controlled trial. Am J Transplant 2007;7:1616–23 - PubMed
-
- Lerut J, Mathys J, Verbaandert C, et al. Tacrolimus monotherapy in liver transplantation: one-year results of a prospective, randomized, double-blind, placebo-controlled study. Ann Surg 2008;248:956–67 - PubMed
-
- Soliman T, Hetz H, Burghuber C, et al. Short-term versus long-term induction therapy with antithymocyte globulin in orthotopic liver transplantation. Transpl Int 2007;20:447–52 - PubMed
-
- Becker T, Foltys D, Bilbao I, et al. Patient outcomes in two steroid-free regimens using tacrolimus monotherapy after daclizumab induction and tacrolimus with mycophenolate mofetil in liver transplantation. Transplantation 2008;86:1689–94 - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
