

Sphenoid masses in children: radiologic differential diagnosis with pathologic correlation
- PMID: 20595365
- PMCID: PMC7965862
- DOI: 10.3174/ajnr.A2144
Sphenoid masses in children: radiologic differential diagnosis with pathologic correlation
Abstract
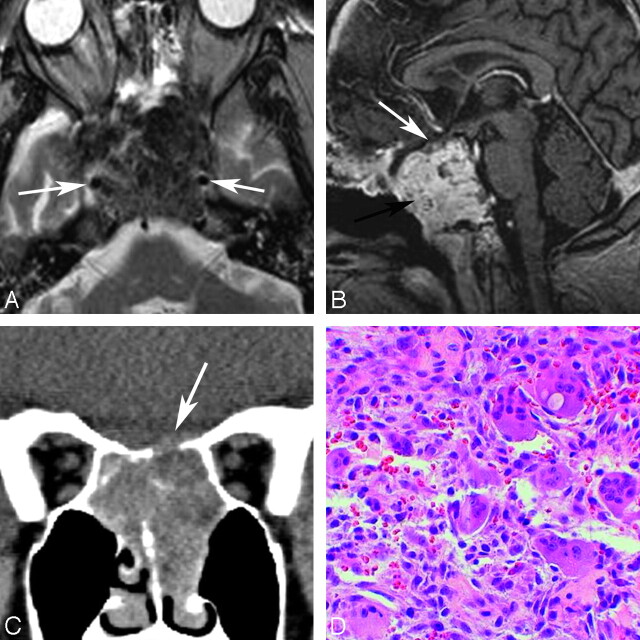
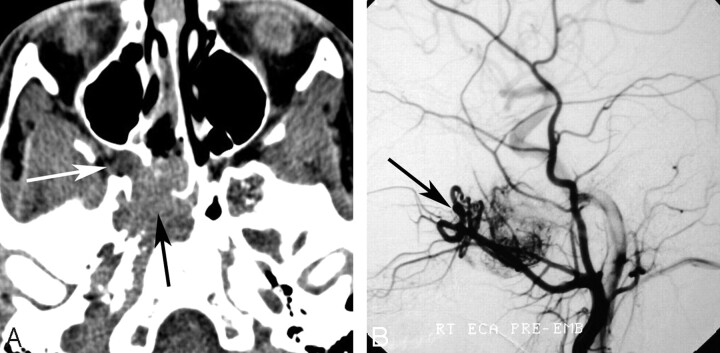
Childhood central skull base masses are rare, often difficult to diagnose, and have overlapping imaging findings. In this review, we provide an overview of the epidemiology, clinical findings, and management of pediatric sphenoid bone and sphenoid sinus masses with an emphasis on imaging findings that may help to differentiate lesions. Radiologic-pathologic correlation is provided. Finally, an imaging-based algorithm is presented as a guide to help radiologists narrow their differential diagnoses. Some of the entities discussed are virtually unique to the pediatric population; others occur rarely in this age group but should be considered in the appropriate clinical setting. Entities included in the discussion are grouped into 2 categories: those that cause nonaggressive osseous remodeling and those that are more commonly associated with aggressive bone changes. Mucocele, aneurysmal bone cyst, giant cell lesions, meningioma, and fibrous dysplasia tend to remodel bone, while entities such as chordoma, craniopharyngioma, rhabdomyosarcoma, sinonasal carcinoma, and neuroblastoma may cause more aggressive local bone changes.
Figures











Similar articles
-
Dumbbell tumor of the anterior skull base. Meningioma? No, adenoid cystic carcinoma!Surg Neurol. 1998 Nov;50(5):470-4. doi: 10.1016/s0090-3019(97)00340-6. Surg Neurol. 1998. PMID: 9842875
-
Imaging the sphenoid bone and basiocciput: pathological considerations.Semin Ultrasound CT MR. 1993 Jun;14(3):160-77. doi: 10.1016/s0887-2171(05)80077-0. Semin Ultrasound CT MR. 1993. PMID: 8357619 Review.
-
Neuroimaging: intrinsic lesions of the central skull base region.Semin Ultrasound CT MR. 2013 Oct;34(5):412-35. doi: 10.1053/j.sult.2013.08.004. Semin Ultrasound CT MR. 2013. PMID: 24216451 Review.
-
[The sphenoid: tumoral pathology].J Neuroradiol. 2003 Sep;30(4):225-37. J Neuroradiol. 2003. PMID: 14566190 French.
-
Telangiectatic osteosarcoma of the skull base.AJNR Am J Neuroradiol. 1998 Apr;19(4):754-7. AJNR Am J Neuroradiol. 1998. PMID: 9576668 Free PMC article.
Cited by
-
Intrasphenoidal Rathke Cleft Cyst: A Rare Case Report.J Pediatr Neurosci. 2021 Oct-Dec;16(4):350-353. doi: 10.4103/jpn.JPN_262_20. Epub 2022 Jan 7. J Pediatr Neurosci. 2021. PMID: 36531764 Free PMC article.
-
Giant Cell Tumor of the Central Skull Base.Cureus. 2024 Sep 17;16(9):e69602. doi: 10.7759/cureus.69602. eCollection 2024 Sep. Cureus. 2024. PMID: 39421119 Free PMC article.
-
Sphenoid sinus pyocele after transsphenoidal approach for pituitary adenoma.Pituitary. 2012 Jun;15(2):188-92. doi: 10.1007/s11102-011-0305-4. Pituitary. 2012. PMID: 21442274 Review.
-
Aneurysmal Bone Cyst of Sphenoid Bone and Clivus Misdiagnosed as Chordoma: A Case Report.Brain Tumor Res Treat. 2015 Oct;3(2):115-7. doi: 10.14791/btrt.2015.3.2.115. Epub 2015 Oct 30. Brain Tumor Res Treat. 2015. PMID: 26605267 Free PMC article.
-
Sphenoid mucocele with unusual panhypopituitarism.BMJ Case Rep. 2016 Apr 5;2016:bcr2015214218. doi: 10.1136/bcr-2015-214218. BMJ Case Rep. 2016. PMID: 27048396 Free PMC article.
References
-
- Levine H. The sphenoid sinus, the neglected nasal sinus. Arch Otolaryngol 1978;104:585–87 - PubMed
-
- Grossman RI, Yousem DM. Neuroradiology: The Requisites. St. Louis:Mosby-Year Book Inc;1994
-
- Alvarez RJ, Liu NJ, Isaacson G. Pediatric ethmoid mucoceles in cystic fibrosis: long-term follow-up of reported cases. Ear Nose Throat J 1997;76:538–39,543–46 - PubMed
-
- Bailey BJ, Johnson JT, Newlands SD, eds. Head & Neck Surgery: Otolaryngology. 4th ed. Philadelphia:Lippincott Williams & Wilkins;2006
-
- Stankiewicz JA. Sphenoid sinus mucocele. Arch Otolaryngol Head Neck Surg 1989;115:735–40 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical