

Cost savings with rapid diagnostic tests for malaria in low-transmission areas: evidence from Dar es Salaam, Tanzania
- PMID: 20595479
- PMCID: PMC2912577
- DOI: 10.4269/ajtmh.2010.09-0632
Cost savings with rapid diagnostic tests for malaria in low-transmission areas: evidence from Dar es Salaam, Tanzania
Abstract
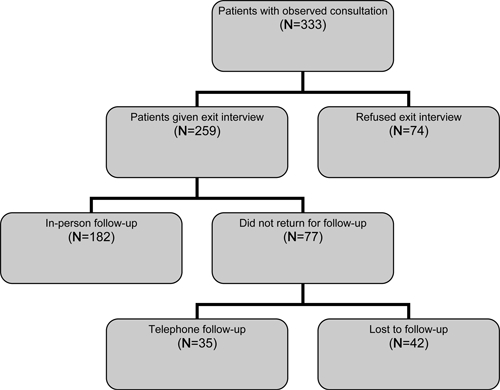
Rapid diagnostic tests (RDTs) for malaria may help rationalize antimalarial drug use. However, the economic effects of these tests may vary. Data on costs were collected from 259 patients in 6 health facilities by using exit and in-charge interviews and record reviews during a trial of RDT rollout in Dar es Salaam, Tanzania. The RDTs decreased patient expenditure on drugs (savings = U.S. $0.36; P = 0.002) and provider drug costs (savings = U.S. $0.43; P = 0.034) compared with control facilities. However, RDT introduction did not significantly reduce patients' overall expenditures (U.S. $1.02, 95% confidence interval [CI] = $0.76-$1.36 versus U.S. $1.33 95% CI = $0.99-$1.77) and may increase total provider costs (U.S. $3.63, 95% CI = $3.40-$3.89 versus U.S. $2.32, 95% CI = $1.99-$2.69) compared with control facilities. Clinician's compliance with test results was higher with RDTs than with routine microscopy (95% versus 82%; P = 0.002). The RDTs reduced drug costs in this setting but did not offset the cost of the tests, although they also resulted in non-monetary benefits, including improved management of patients and increased compliance with test results.
Conflict of interest statement
Disclosure: The main sponsoring institution (Swiss National Science Foundation) had no role in the study design, data collection, data analysis, data interpretation or writing of this report. All authors had full access to all study data.
Figures
Similar articles
-
Use of HRP-2-based rapid diagnostic test for Plasmodium falciparum malaria: assessing accuracy and cost-effectiveness in the villages of Dielmo and Ndiop, Senegal.Malar J. 2010 Jun 4;9:153. doi: 10.1186/1475-2875-9-153. Malar J. 2010. PMID: 20525322 Free PMC article.
-
Cost-effectiveness analysis of rapid diagnostic test, microscopy and syndromic approach in the diagnosis of malaria in Nigeria: implications for scaling-up deployment of ACT.Malar J. 2009 Nov 23;8:265. doi: 10.1186/1475-2875-8-265. Malar J. 2009. PMID: 19930666 Free PMC article.
-
Cost-effectiveness of malaria diagnosis using rapid diagnostic tests compared to microscopy or clinical symptoms alone in Afghanistan.Malar J. 2015 May 28;14:217. doi: 10.1186/s12936-015-0696-1. Malar J. 2015. PMID: 26016871 Free PMC article. Clinical Trial.
-
Interpreting rapid diagnostic test (RDT) for Plasmodium falciparum.BMC Res Notes. 2018 Dec 4;11(1):850. doi: 10.1186/s13104-018-3967-4. BMC Res Notes. 2018. PMID: 30509313 Free PMC article. Review.
-
Costs and financial feasibility of malaria elimination.Lancet. 2010 Nov 6;376(9752):1604-15. doi: 10.1016/S0140-6736(10)61355-4. Epub 2010 Oct 28. Lancet. 2010. PMID: 21035839 Free PMC article. Review.
Cited by
-
Major reduction in anti-malarial drug consumption in Senegal after nation-wide introduction of malaria rapid diagnostic tests.PLoS One. 2011 Apr 6;6(4):e18419. doi: 10.1371/journal.pone.0018419. PLoS One. 2011. PMID: 21494674 Free PMC article.
-
Incorporating Demand and Supply Constraints into Economic Evaluations in Low-Income and Middle-Income Countries.Health Econ. 2016 Feb;25 Suppl 1(Suppl Suppl 1):95-115. doi: 10.1002/hec.3306. Epub 2016 Jan 19. Health Econ. 2016. PMID: 26786617 Free PMC article.
-
The epidemiology of residual Plasmodium falciparum malaria transmission and infection burden in an African city with high coverage of multiple vector control measures.Malar J. 2016 May 23;15(1):288. doi: 10.1186/s12936-016-1340-4. Malar J. 2016. PMID: 27216734 Free PMC article.
-
Malaria diagnosis in rural healthcare facilities and treatment-seeking behavior in malaria endemic settings in western Kenya.PLOS Glob Public Health. 2023 Jul 20;3(7):e0001532. doi: 10.1371/journal.pgph.0001532. eCollection 2023. PLOS Glob Public Health. 2023. PMID: 37471336 Free PMC article.
-
Spatial heterogeneity can undermine the effectiveness of country-wide test and treat policy for malaria: a case study from Burkina Faso.Malar J. 2016 Oct 19;15(1):513. doi: 10.1186/s12936-016-1565-2. Malar J. 2016. PMID: 27760546 Free PMC article.
References
-
- World Health Organization . World Malaria Report 2008. Geneva: World Health Organization; 2008. WHO/HTM/GMP/2008.1. 2008.
-
- Mundy C, Ngwira M, Kadewele G, Bates I, Squire SB, Gilks CF. Evaluation of microscope condition in Malawi. Trans R Soc Trop Med Hyg. 2000;94:583–584. - PubMed
-
- Kahama-Maro J, D'Acremont V, Mtasiwa D, Genton B, Lengeler C. Low quality of routine microscopy for malaria at different health system levels in Dar es Salaam: rapid diagnostic tests should also be implemented in hospitals and urban settings. Abstract book of the 57th Annual Meeting of the American Society of Tropical Medicine and Hygiene. New Orleans; Louisiana: 2008. December 7–11.
-
- Bell D, Peeling RW. Evaluation of rapid diagnostic tests: malaria. Nat Rev Microbiol. 2006;4((Suppl)):S34–S38. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
