

Far cortical locking can improve healing of fractures stabilized with locking plates
- PMID: 20595573
- PMCID: PMC2897208
- DOI: 10.2106/JBJS.I.01111
Far cortical locking can improve healing of fractures stabilized with locking plates
Abstract
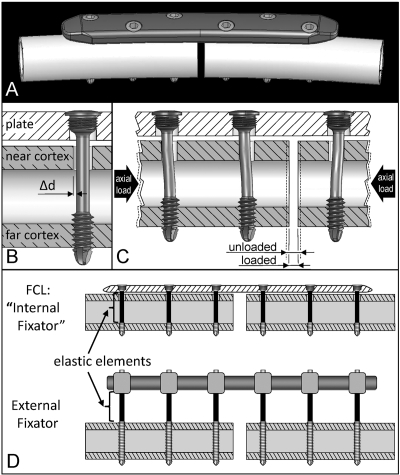
Background: Locked bridge plating relies on secondary bone healing, which requires interfragmentary motion for callus formation. This study evaluated healing of fractures stabilized with a locked plating construct and a far cortical locking construct, which is a modified locked plating approach that promotes interfragmentary motion. The study tested whether far cortical locking constructs can improve fracture-healing compared with standard locked plating constructs.
Methods: In an established ovine tibial osteotomy model with a 3-mm gap size, twelve osteotomies were randomly stabilized with locked plating or far cortical locking constructs applied medially. The far cortical locking constructs were designed to provide 84% lower stiffness than the locked plating constructs and permitted nearly parallel gap motion. Fracture-healing was monitored on weekly radiographs. After the animals were killed at week 9, healed tibiae were analyzed by computed tomography, mechanical testing in torsion, and histological examination.
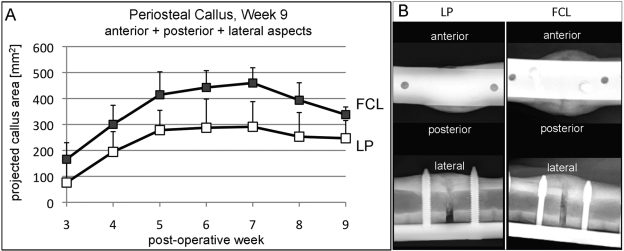
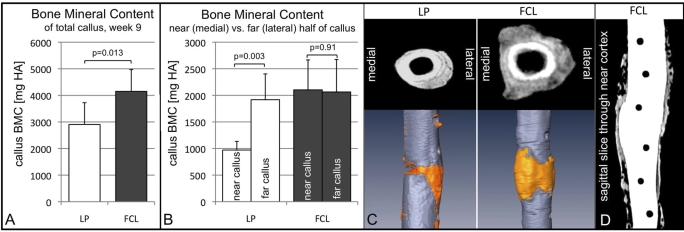
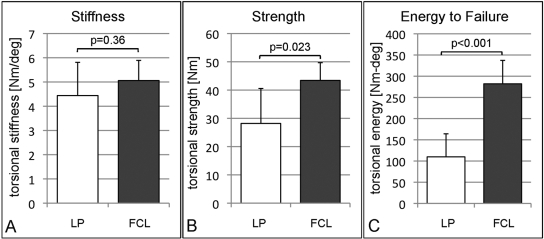
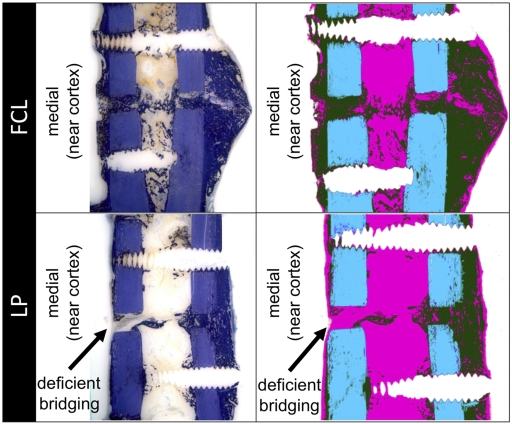
Results: Callus on weekly radiographs was greater in the far cortical locking constructs than in the locked plating constructs. At week 9, the far cortical locking group had a 36% greater callus volume (p = 0.03) and a 44% higher bone mineral content (p = 0.013) than the locked plating group. Callus in the locked plating specimens was asymmetric, having 49% less bone mineral content in the medial callus than in the lateral callus (p = 0.003). In far cortical locking specimens, medial and lateral callus had similar bone mineral content (p = 0.91). The far cortical locking specimens healed to be 54% stronger in torsion (p = 0.023) and sustained 156% greater energy to failure in torsion (p < 0.001) than locked plating specimens. Histologically, three of six locked plating specimens had deficient bridging across the medial cortex, while all remaining cortices had bridged.
Conclusions: Inconsistent and asymmetric callus formation with locked plating constructs is likely due to their high stiffness and asymmetric gap closure. By providing flexible fixation and nearly parallel interfragmentary motion, far cortical locking constructs form more callus and heal to be stronger in torsion than locked plating constructs.
Figures
References
-
- Kubiak EN, Fulkerson E, Strauss E, Egol KA. The evolution of locked plates. J Bone Joint Surg Am. 2006;88Suppl 4:189-200 - PubMed
-
- Ring D, Kloen P, Kadzielski J, Helfet D, Jupiter JB. Locking compression plates for osteoporotic nonunions of the diaphyseal humerus. Clin Orthop Relat Res. 2004;425:50-4 - PubMed
-
- Perren SM. Evolution of the internal fixation of long bone fractures. The scientific basis of biological internal fixation: choosing a new balance between stability and biology. J Bone Joint Surg Br. 2002;84:1093-110 - PubMed
-
- Tan SL, Balogh ZJ. Indications and limitations of locked plating. Injury. 2009;40:683-91 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
