

Current state of neck dissection in the United States
- PMID: 20596978
- PMCID: PMC2811628
- DOI: 10.1007/s12105-009-0129-y
Current state of neck dissection in the United States
Abstract
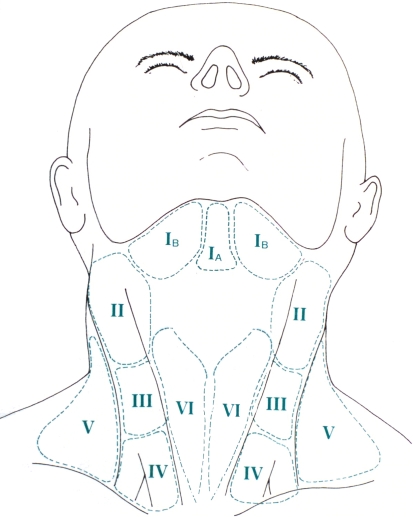
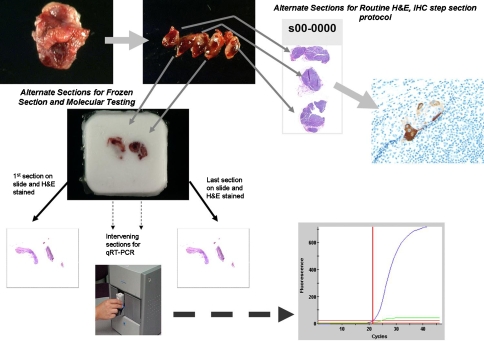
The status of the cervical lymph nodes is the most important prognosticator in head and neck squamous cell carcinoma. The neck dissection is both a therapeutic and staging procedure and has evolved to include various types with standardized level designations (I-VI) for lymph node groups: the radical neck dissection, modified radical neck dissection, the selective neck dissection, and the extended neck dissection. The gross and histologic examination of a neck dissection should provide the critical information (size of metastasis, number of lymph nodes involved) for staging purposes. Additionally, extracapsular spread of lymph node metastasis must be reported because of its significance as an adverse prognosticator. Current dilemmas in nodal disease are the detection of micrometastases, isolated tumor cells, and molecular positivity. The significance of these categories of disease is still unclear, though they may explain a subset of the estimated 10% of the regional recurrences in the neck despite pathologic node negativity by traditional methods of evaluation. Sentinel lymph node biopsy has been recently applied to head and neck squamous cell carcinoma to enhance the management of the clinicoradiographically node negative patients. While still investigational, sentinel lymph node biopsy shows promise in selecting patients who require a neck dissection. Rapid highly automated real-time RT-PCR based platforms will allow for incorporation of molecular findings into the intraoperative evaluation of a sentinel lymph node.
Figures
Similar articles
-
Rapid molecular detection of metastatic head and neck squamous cell carcinoma as an intraoperative adjunct to sentinel lymph node biopsy.Laryngoscope. 2012 May;122(5):1020-30. doi: 10.1002/lary.22467. Epub 2012 Mar 23. Laryngoscope. 2012. PMID: 22447185 Free PMC article.
-
Neck dissection: then and now.Auris Nasus Larynx. 2006 Dec;33(4):365-74. doi: 10.1016/j.anl.2006.06.001. Epub 2006 Aug 4. Auris Nasus Larynx. 2006. PMID: 16889923 Review.
-
The impact of sentinel lymph node biopsy on the quality of life in patients with oral cavity squamous cell carcinoma.Braz J Otorhinolaryngol. 2022 May-Jun;88(3):434-438. doi: 10.1016/j.bjorl.2020.11.015. Epub 2020 Dec 27. Braz J Otorhinolaryngol. 2022. PMID: 33422480 Free PMC article.
-
Elective neck dissection in oral carcinoma: a critical review of the evidence.Acta Otorhinolaryngol Ital. 2007 Jun;27(3):113-7. Acta Otorhinolaryngol Ital. 2007. PMID: 17883186 Free PMC article. Review.
-
The role of neck dissection in squamous cell carcinoma of the head and neck.Curr Treat Options Oncol. 2014 Dec;15(4):611-24. doi: 10.1007/s11864-014-0311-7. Curr Treat Options Oncol. 2014. PMID: 25228145 Review.
Cited by
-
Focus issue: neck dissection for oropharyngeal squamous cell carcinoma.ISRN Surg. 2012;2012:547017. doi: 10.5402/2012/547017. Epub 2012 Jan 15. ISRN Surg. 2012. PMID: 22586518 Free PMC article.
-
Correlation of tumor marker expression with nodal disease burden in metastatic head and neck cancer.Otolaryngol Head Neck Surg. 2013 Aug;149(2):261-8. doi: 10.1177/0194599813486876. Epub 2013 Apr 26. Otolaryngol Head Neck Surg. 2013. PMID: 23625795 Free PMC article.
-
Effectiveness and pitfalls of elective neck dissection in N0 laryngeal cancer.Acta Otorhinolaryngol Ital. 2011 Aug;31(4):216-21. Acta Otorhinolaryngol Ital. 2011. PMID: 22058599 Free PMC article.
-
Optical molecular imaging can differentiate metastatic from benign lymph nodes in head and neck cancer.Nat Commun. 2019 Nov 6;10(1):5044. doi: 10.1038/s41467-019-13076-7. Nat Commun. 2019. PMID: 31695030 Free PMC article.
-
A pilot study of quantitative real-time polymerase chain reaction metastases detection on sentinel lymph nodes of oral cancer and literature review.Rev Assoc Med Bras (1992). 2024 Jun 7;70(suppl 1):e2024S126. doi: 10.1590/1806-9282.2024S126. eCollection 2024. Rev Assoc Med Bras (1992). 2024. PMID: 38865545 Free PMC article. Review. No abstract available.
References
-
- Robbins KT, Clayman G, Levine PA, et al. Neck dissection classification update: revisions proposed by the American Head and Neck Society and the American Academy of Otolaryngology–Head and Neck Surgery. Arch Otolaryngol Head Neck Surg. 2002;128(7):751–758. - PubMed
-
- AJCC Cancer Staging Manual. 6th ed. Springer; 2002.
-
- Beldi D, Jereczek-Fossa BA, D’Onofrio A, et al. Role of radiotherapy in the treatment of cervical lymph node metastases from an unknown primary site: retrospective analysis of 113 patients. Int J Radiat Oncol Biol Phys. 2007;69(4):1051–1058. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
