

Update to the College of American Pathologists reporting on thyroid carcinomas
- PMID: 20596997
- PMCID: PMC2807537
- DOI: 10.1007/s12105-009-0109-2
Update to the College of American Pathologists reporting on thyroid carcinomas
Abstract
Background: The reporting of thyroid carcinomas follows the recommendations of the College of American Pathologists (CAP) protocols and includes papillary carcinoma, follicular carcinoma, anaplastic carcinoma and medullary carcinoma. Despite past and recent efforts, there are a number of controversial issues in the classification and diagnosis of thyroid carcinomas (TC) that, potentially impact on therapy and prognosis of patients with TC.
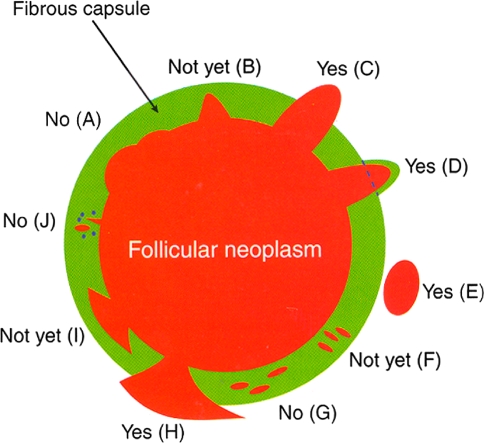
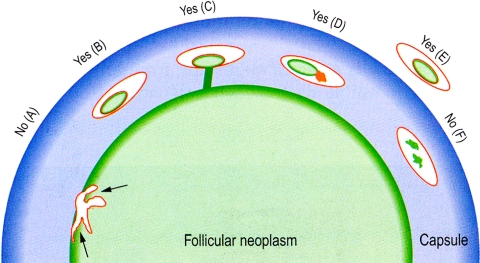
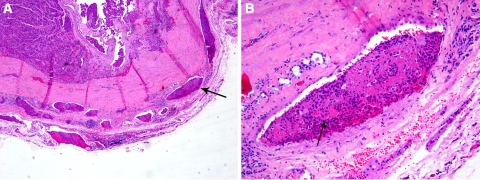
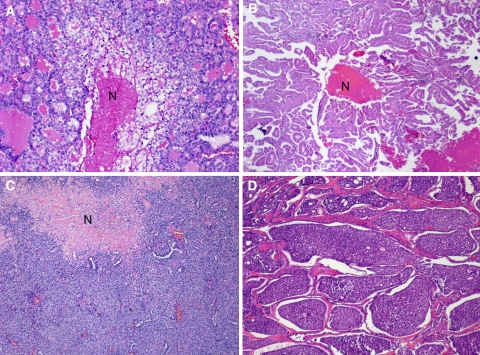
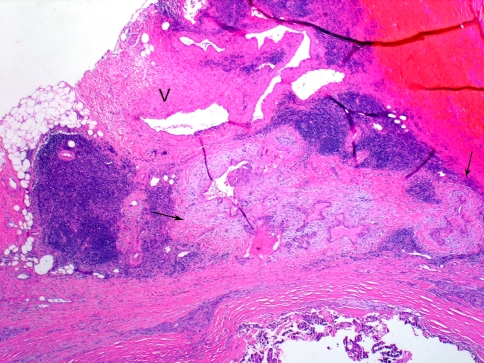
Discussion: The most updated version of the CAP thyroid cancer protocol incorporates recent changes in histologic classification as well as changes in the staging of thyroid cancers as per the updated American Joint Commission on Cancer staging manual. Among the more contentious issues in the pathology of thyroid carcinoma include the defining criteria for tumor invasiveness. While there are defined criteria for invasion, there is not universal agreement in what constitutes capsular invasion, angioinvasion and extrathyroidal invasion. Irrespective of the discrepant views on invasion, pathologists should report on the presence and extent (focal, widely) of capsular invasion, angioinvasion and extrathyroidal extension. These findings assist clinicians in their assessment of the recurrence risk and potential for metastatic disease. It is beyond the scope of this paper to detail the entire CAP protocol for thyroid carcinomas; rather, this paper addresses some of the more problematic issues confronting pathologists in their assessment and reporting of thyroid carcinomas.
Conclusion: The new CAP protocol for reporting of thyroid carcinomas is a step toward improving the clinical value of the histopathologic reporting of TC. Large meticulous clinico-pathologic and molecular studies with long term follow up are still needed in order to increase the impact of microscopic examination on the prognosis and management of TC.
Keywords: CAP; Capsular; Carcinoma; Extension; Extrathyroid; Invasion; Margins; Minimally invasive; Mitosis; Necrosis; Papillary microcarcinomas; Reporting; Thyroid; Vascular; Widely invasive.
Figures
References
-
- Chan JKC. Tumors of the thyroid and parathyroid glands. In: Fletcher CDM, editor. Diagnostic Histopathology of Tumors. 3. London, England: Churchill Livingston; 2007. pp. 997–1078.
-
- Rosai J, Carcangiu ML, Delellis RA. Tumors of the Thyroid Gland, Atlas of Tumor Pathology. Washington DC: Armed Forces Institute of Pathology; 1992.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
