

Disparities in maternal hypertension and pregnancy outcomes: evidence from North Carolina, 1994-2003
- PMID: 20597458
- PMCID: PMC2882609
- DOI: 10.1177/003335491012500413
Disparities in maternal hypertension and pregnancy outcomes: evidence from North Carolina, 1994-2003
Abstract
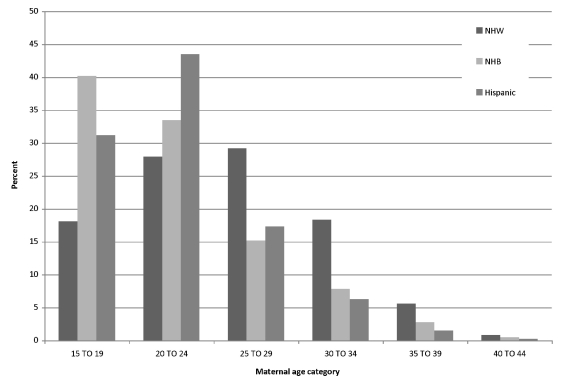
Objectives: To better understand disparities in pregnancy outcomes, we analyzed data from North Carolina to determine how the pattern of maternal hypertensive disorders differs among non-Hispanic white (NHW), non-Hispanic black (NHB), and Hispanic women across the range of maternal ages. In addition, we explored whether rates of poor birth outcomes, including low birthweight (LBW) and preterm birth (PTB), among hypertensive women differed by race.
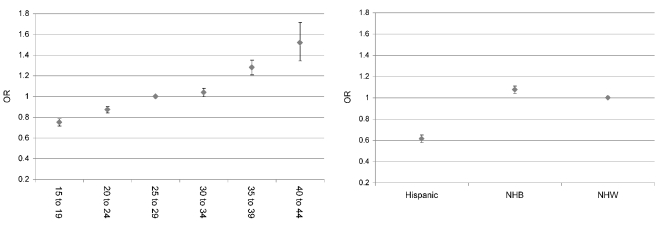
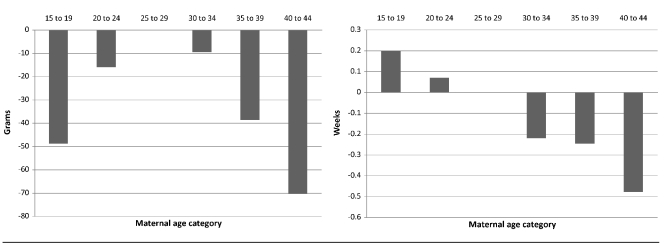
Methods: We restricted our analyses to births occurring between 1994 and 2003, constructing six five-year maternal age categories: 15-19 years, 20-24 years, 25-29 years, 30-34 years, 35-39 years, and 40-44 years. We used logistic regression to determine the relative contribution of race and age to incidence of maternal hypertension. All analyses controlled for the standard covariates of maternal education, marital status, and tobacco use. To assess the impact of maternal hypertension on birth outcomes, we limited the dataset to women with any hypertensive disorder and used linear regression to determine how particular race-age combinations affected outcomes. We also used logistic regression to find out how particular race-age combinations affected the likelihood of LBW and PTB.
Results: The risk of hypertension differed by race, with NHB women exhibiting the highest risk and Hispanic women the lowest risk. Further, rates of hypertension increased with age. Among hypertensive women, pregnancy outcomes differed by race and age, with NHB women having the poorest outcomes (i.e., LBW and PTB) and age exhibiting a dose-response relationship in PTB and very PTB.
Conclusions: Patterns of maternal hypertension and subsequent outcomes are important contributors to persistent disparities in pregnancy outcomes.
Figures
References
-
- Johnston RB, Jr, Williams MA, Hogue CJ, Mattison DR. Overview: new perspectives on the stubborn challenge of preterm birth. Paediatr Perinat Epidemiol. 2001;15(Suppl 2):3–6. - PubMed
-
- Wise PH, Kotelchuck M, Wilson ML, Mills M. Racial and socioeconomic disparities in childhood mortality in Boston. N Engl J Med. 1985;313:360–6. - PubMed
-
- Martin JA, Hamilton BE, Sutton PD, Ventura SJ, Menacker F, Kirmeyer S, et al. Births: final data for 2006. Natl Vital Stat Rep. 2009 Jan 7;57:1–104. - PubMed
-
- Mathews TJ, MacDorman MF. Infant mortality statistics from the 2005 period linked birth/infant death data set. Natl Vital Stat Rep. 2008 Jul 30;57:1–32. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
