

Bone metastases from renal cell carcinoma: patient survival after surgical treatment
- PMID: 20598157
- PMCID: PMC2909163
- DOI: 10.1186/1471-2474-11-145
Bone metastases from renal cell carcinoma: patient survival after surgical treatment
Abstract
Background: Surgery is the primary treatment of skeletal metastases from renal cell carcinoma, because radiation and chemotherapy frequently are not effecting the survival. We therefore explored factors potentially affecting the survival of patients after surgical treatment.
Methods: We retrospectively reviewed 101 patients operatively treated for skeletal metastases of renal cell carcinoma between 1980 and 2005. Overall survival was calculated using the Kaplan-Meier method. The effects of different variables were evaluated using a log-rank test.
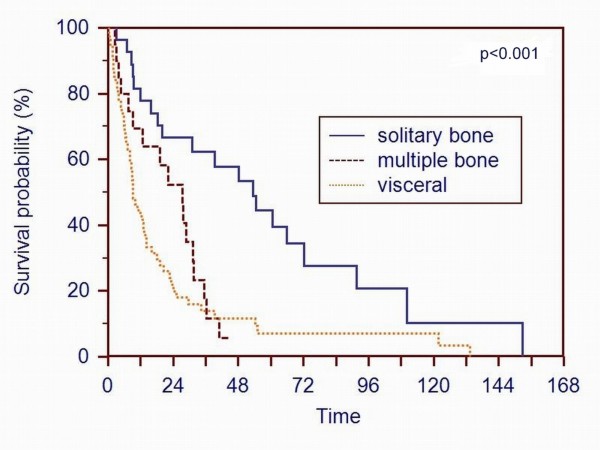
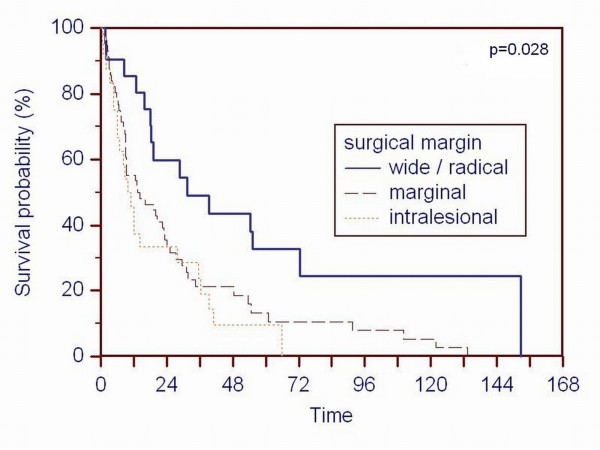
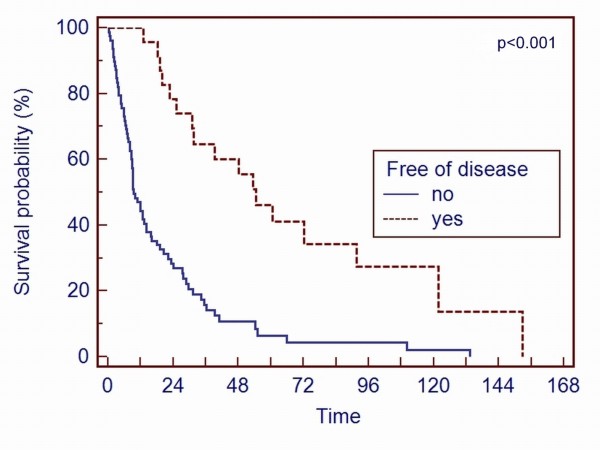
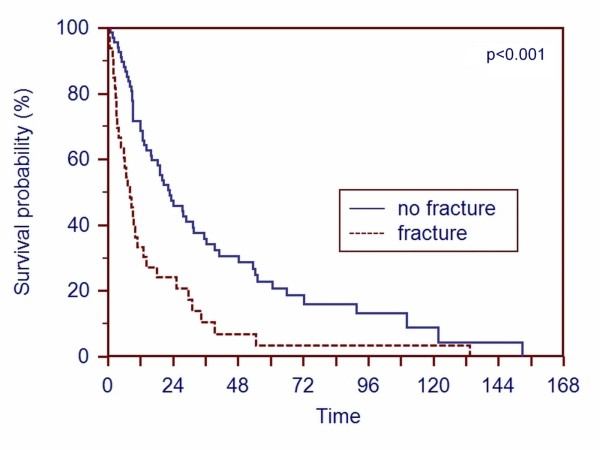
Results: 27 patients had a solitary bone metastasis, 20 patients multiple bone metastases and 54 patients had concomitant visceral metastases. The overall survival was 58% at 1 year, 37% at 2 years and 12% at 5 years. Patients with solitary bone metastases had a better survival (p < 0.001) compared to patients with multiple metastases. Age younger than 65 years (p = 0.036), absence of pathologic fractures (p < 0.001) and tumor-free resection margins (p = 0.028) predicted higher survival. Gender, location of metastases, time between diagnosis of renal cell carcinoma and treatment of metastatic disease, incidence of local recurrence, radiation and chemotherapy did not influence survival.
Conclusions: The data suggest that patients with a solitary metastasis or a limited number of resectable metastases are candidates for wide resections. As radiation and chemotherapy are ineffective in most patients, surgery is a better option to achieve local tumor control and increase the survival.
Figures
References
-
- McLaughlin JK, Lipworth L. Epidemiologic aspects of renal cell cancer. Semin Oncol. 2000;27:115–123. - PubMed
-
- Patard JJ, Kim HL, Lam JS, Dorey FJ, Pantuck AJ, Zisman A, Ficarra V, Han KR, Cindolo L, De La Taille A, Tostain J, Artibani W, Dinney CP, Wood CG, Swanson DA, Abbou CC, Lobel B, Mulders PF, Chopin DK, Figlin RA, Belldegrun AS. Use of the University of California Los Angeles integrated staging system to predict survival in renal cell carcinoma: an international multicenter study. J Clin Oncol. 2004;15;22(16):3316–22. doi: 10.1200/JCO.2004.09.104. - DOI - PubMed
-
- Han KR, Pantuck AJ, Bui MH, Shvarts O, Freitas DG, Zisman A, Leibovich BC, Dorey FJ, Gitlitz BJ, Figlin RA, Belldegrun AS. Number of metastatic sites rather than location dictates overall survival of patients with node-negative metastatic renal cell carcinoma. Urology. 2003;61(2):314–9. doi: 10.1016/S0090-4295(02)02163-5. - DOI - PubMed
-
- Zekri J, Ahmed N, Coleman RE, Hancock BW. The skeletal metastatic compli cations of renal cell carcinoma. Int J Oncol. 2001;19(2):379–82. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
