

Growth hormone status predicts left ventricular mass in patients after cure of acromegaly
- PMID: 20598930
- PMCID: PMC3670701
- DOI: 10.1016/j.ghir.2010.05.003
Growth hormone status predicts left ventricular mass in patients after cure of acromegaly
Abstract
Context: Growth hormone excess and growth hormone deficiency (GHD) are both associated with increased cardiovascular morbidity. A specific acromegaly-related cardiomyopathy has been described, characterized in part by increased left ventricular mass (LVM). Growth hormone deficiency is associated with reduced LVM. Following cure of acromegaly with surgery or radiation therapy, GHD may develop; however, its effects on cardiac morphology and function in this population are not established.
Objective: We hypothesized that the development of GHD in patients with prior acromegaly would be associated with cardiac morphologic and functional changes that differ from those in patients who are GH sufficient following cure of acromegaly.
Design: A cross-sectional study was conducted in a Clinical Research Center. Study participants consisted of three groups of subjects (n=34): I. Cured acromegaly with GHD (n=15), II. Cured acromegaly with GH sufficiency (n=8), and III. Active acromegaly (n=11). Main outcome measures included cardiac morphology and function, using echocardiography parameters.
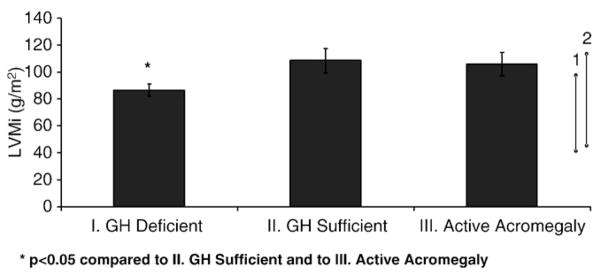
Results: Mean age and BMI, 44.6 ± 2.3 years (SEM) and 30.7 ± 1.3 kg/m², respectively, were not different among the three groups. Mean peak GH values were: I. 2.8 ± 0.4 ng/ml; II. 30.1 ± 9.1 ng/ml (p=0.0002.) In group I, left ventricular mass, indexed to body surface area (LVMi), was within the normal range in all patients; moreover, left ventricular (LV) geometry was normal. At least 50% of patients in groups II and III had elevated LVMi, and in 50% of patients, LV geometry was abnormal, indicating pathologic hypertrophy. Ejection fraction was similar between all three groups. There were no significant differences in diastolic function.
Conclusions: Patients who develop GHD following cure of acromegaly do not demonstrate elevated LV mass, in contrast to patients with a history of acromegaly but normal GH levels or to patients with active acromegaly. This suggests that GH status after treatment of acromegaly correlates with LV mass, and that, in GH sufficient patients, reversal of remodeling may be slower than previously thought. These data suggest that it will be important to determine whether GH replacement alters left ventricular morphology over time.
Copyright © 2010 Growth Hormone Research Society. Published by Elsevier Ltd. All rights reserved.
Figures
References
-
- Rajasoorya C, Holdaway IM, Wrightson P, Scott DJ, Ibbertson HK. Determinants of clinical outcome and survival in acromegaly. Clin Endocrinol (Oxf) 1994;41:95–102. - PubMed
-
- Holdaway IM. Excess mortality in acromegaly. Horm Res. 2007;68(Suppl 5):166–172. - PubMed
-
- Swearingen B, Barker FG, 2nd, Katznelson L, et al. Long-term mortality after transsphenoidal surgery and adjunctive therapy for acromegaly. J Clin Endocrinol Metab. 1998;83:3419–3426. - PubMed
-
- Holdaway IM, Rajasoorya RC, Gamble GD. Factors influencing mortality in acromegaly. J Clin Endocrinol Metab. 2004;89:667–674. - PubMed
-
- Clayton RN. Cardiovascular function in acromegaly. Endocr Rev. 2003;24:272–277. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
