

Proteomic identification of early biomarkers of acute kidney injury after cardiac surgery in children
- PMID: 20599305
- PMCID: PMC2943007
- DOI: 10.1053/j.ajkd.2010.04.014
Proteomic identification of early biomarkers of acute kidney injury after cardiac surgery in children
Abstract
Background: Serum creatinine is a delayed marker of acute kidney injury (AKI). Our purpose is to discover and validate novel early urinary biomarkers of AKI after cardiac surgery.
Study design: Diagnostic test study.
Setting & participants: Children undergoing cardiopulmonary bypass surgery. The test set included 15 participants with AKI and 15 matched controls (median age, 1.5 year) of 45 participants without AKI. The validation set included 365 children (median age, 1.9 year).
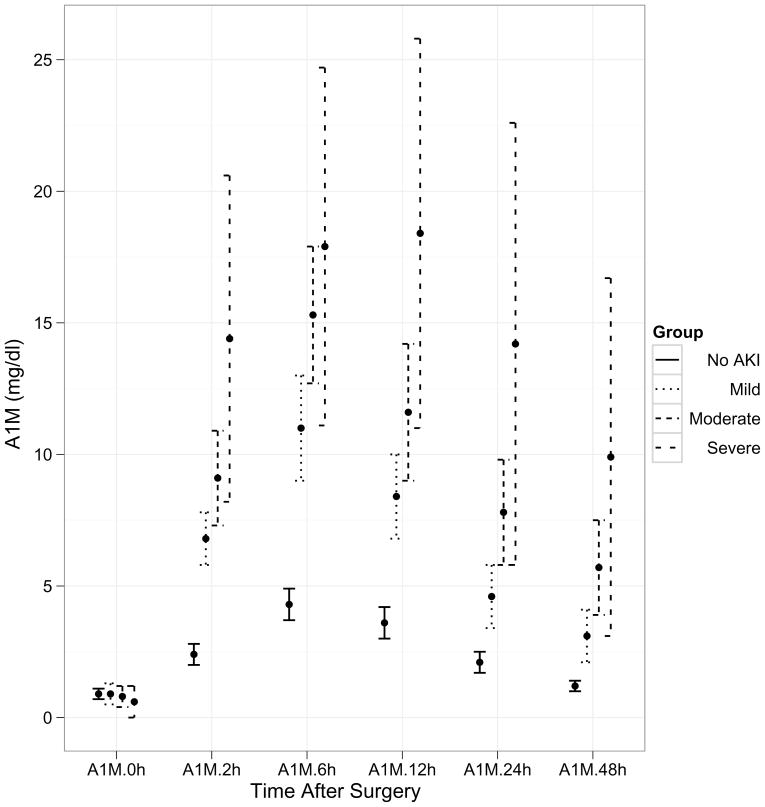
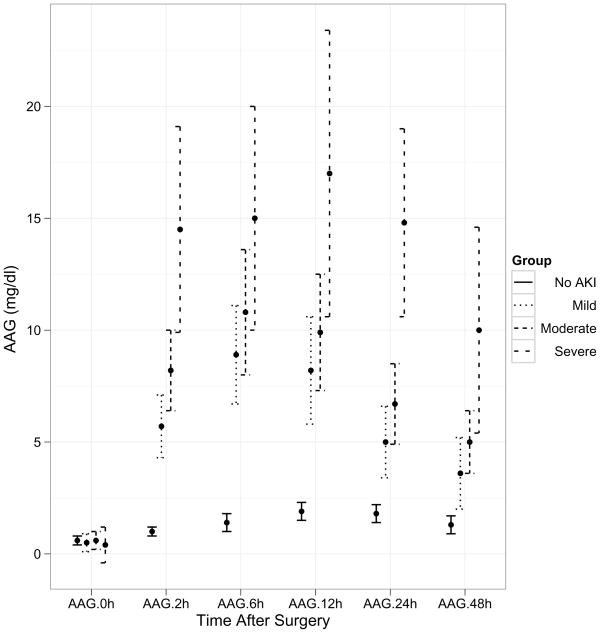
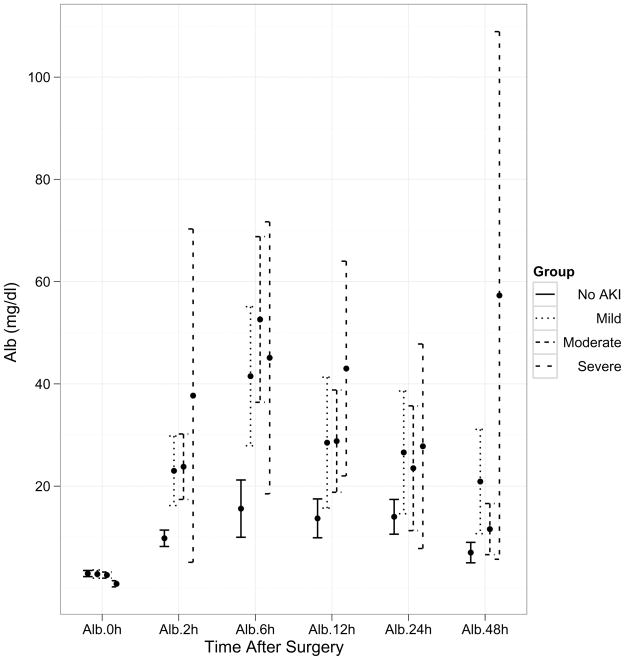
Index tests: Biomarkers identified using proteomic profiling: α(1)-microglobulin, α(1)-acid glycoprotein, and albumin.
Reference test: AKI, defined as ≥50% increase in serum creatinine level from baseline within 3 days of surgery.
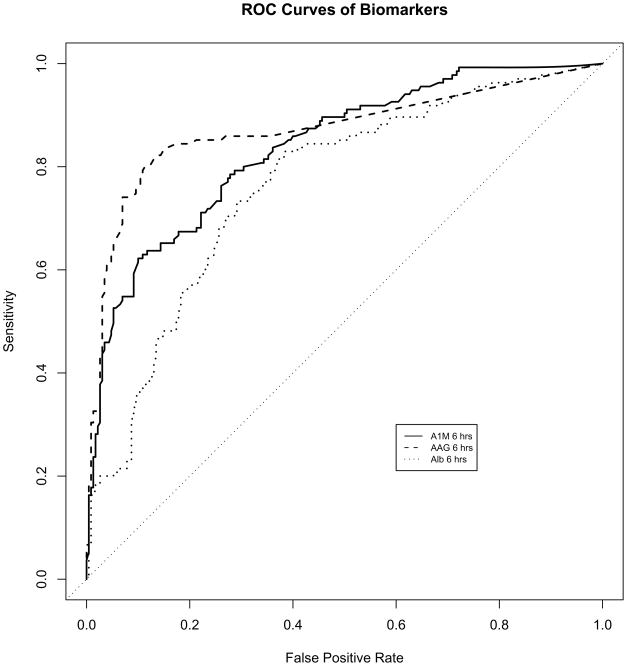
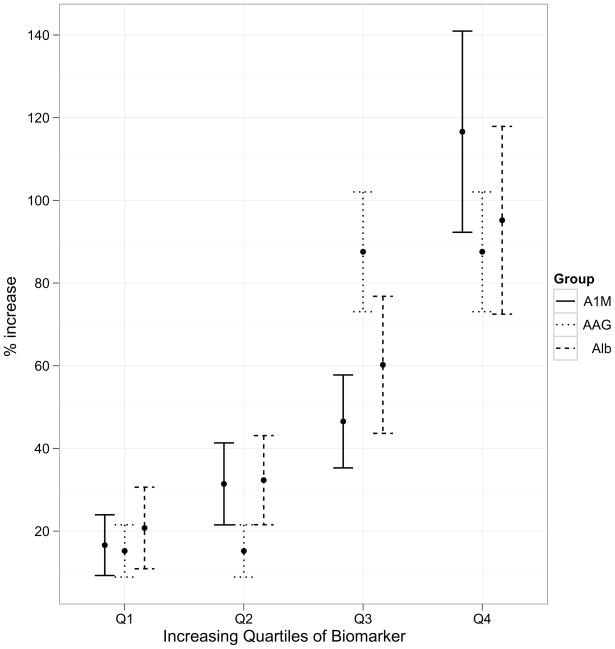
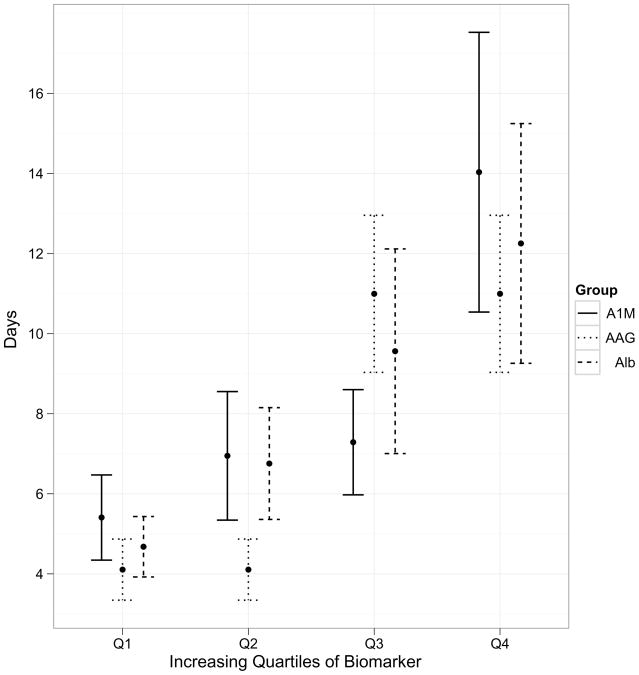
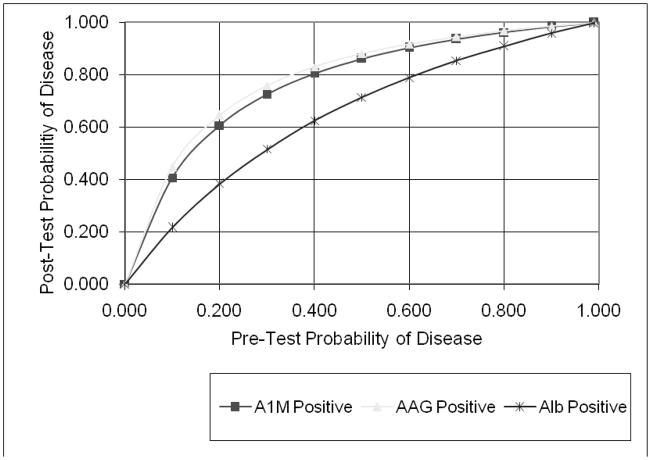
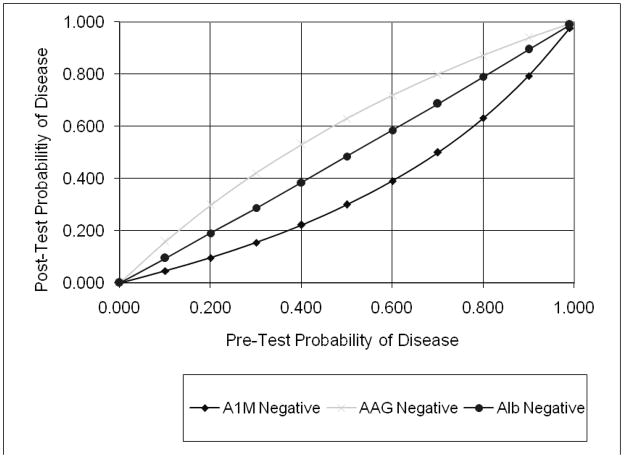
Results: Proteomic profiling using surface-enhanced laser desorption/ionization time-of-flight mass spectrometry (SELDI-TOF MS) showed 3 protein peaks that appeared consistently within 2 hours in children who developed AKI after cardiopulmonary bypass surgery. The proteins were identified as α(1)-microglobulin, α(1)-acid glycoprotein, and albumin. Using clinical assays, results were confirmed in a test set and validated in an independent prospective cohort. In the validation set, 135 (37%) developed AKI, in whom there was a progressive increase in urinary biomarker concentrations with severity of AKI. Areas under the curve for urinary α(1)-microglobulin, α(1)-acid glycoprotein, and albumin at 6 hours after cardiac surgery were 0.84 (95% CI, 0.79-0.89), 0.87 (95% CI, 0.83-0.91), and 0.76 (95% CI, 0.71-0.81), respectively. Participants with increasing quartiles of biomarkers showed increasing lengths of hospital stays and durations of AKI (P < 0.001).
Limitations: Single-center study of children with normal kidney function at recruitment. The SELDI-TOF MS technique has limited sensitivity for the detection of proteins greater than the 20-kDa range.
Conclusions: Urinary α(1)-microglobulin, α(1)-acid glycoprotein, and albumin represent early, accurate, inexpensive, and widely available biomarkers of AKI after cardiac surgery. They also offer prognostic information about the duration of AKI and length of hospitalization after cardiac surgery.
Copyright © 2010 National Kidney Foundation, Inc. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Urinary biomarkers in acute kidney injury: ready for prime time?Am J Kidney Dis. 2010 Oct;56(4):609-11. doi: 10.1053/j.ajkd.2010.08.004. Am J Kidney Dis. 2010. PMID: 20851316 No abstract available.
-
Antifibrinolytic use during cardiac and hepatic surgery makes tubular proteinuria-based early biomarkers poor tools to diagnose perioperative acute kidney injury.Am J Kidney Dis. 2011 Jun;57(6):960; author reply 960-1. doi: 10.1053/j.ajkd.2011.04.005. Am J Kidney Dis. 2011. PMID: 21601130 No abstract available.
Similar articles
-
Mass spectrometry-based proteomic analysis of urine in acute kidney injury following cardiopulmonary bypass: a nested case-control study.Am J Kidney Dis. 2009 Apr;53(4):584-95. doi: 10.1053/j.ajkd.2008.10.037. Epub 2008 Dec 13. Am J Kidney Dis. 2009. PMID: 19070948
-
Comparison of urinary biomarkers for early detection of acute kidney injury after cardiopulmonary bypass surgery in infants and young children.Pediatr Cardiol. 2013 Apr;34(4):880-6. doi: 10.1007/s00246-012-0563-6. Epub 2012 Nov 3. Pediatr Cardiol. 2013. PMID: 23124320
-
Validation of clinical scores predicting severe acute kidney injury after cardiac surgery.Am J Kidney Dis. 2010 Oct;56(4):623-31. doi: 10.1053/j.ajkd.2010.04.017. Epub 2010 Jul 13. Am J Kidney Dis. 2010. PMID: 20630639
-
Congenital heart surgery and acute kidney injury.Curr Opin Anaesthesiol. 2017 Feb;30(1):105-112. doi: 10.1097/ACO.0000000000000406. Curr Opin Anaesthesiol. 2017. PMID: 27748669 Review.
-
Urinary glutathione S-transferases in the pathogenesis and diagnostic evaluation of acute kidney injury following cardiac surgery: a critical review.Curr Opin Crit Care. 2010 Dec;16(6):550-5. doi: 10.1097/MCC.0b013e32833fdd9a. Curr Opin Crit Care. 2010. PMID: 20930627 Free PMC article. Review.
Cited by
-
Three feasible strategies to minimize kidney injury in 'incipient AKI'.Nat Rev Nephrol. 2013 Aug;9(8):484-90. doi: 10.1038/nrneph.2013.80. Epub 2013 May 7. Nat Rev Nephrol. 2013. PMID: 23649020 Review.
-
Early detection of acute kidney injury after pediatric cardiac surgery.Prog Pediatr Cardiol. 2016 Jun;41:9-16. doi: 10.1016/j.ppedcard.2016.01.011. Prog Pediatr Cardiol. 2016. PMID: 27429538 Free PMC article.
-
A benzimidazole inhibitor attenuates sterile inflammation induced in a model of systemic autoinflammation in female mice.Sci Rep. 2020 Jul 21;10(1):12100. doi: 10.1038/s41598-020-68985-1. Sci Rep. 2020. PMID: 32694575 Free PMC article.
-
Marking renal injury: can we move beyond serum creatinine?Transl Res. 2012 Apr;159(4):277-89. doi: 10.1016/j.trsl.2012.01.014. Epub 2012 Feb 3. Transl Res. 2012. PMID: 22424431 Free PMC article. Review.
-
Renal injury in neonates: use of "omics" for developing precision medicine in neonatology.Pediatr Res. 2017 Jan;81(1-2):271-276. doi: 10.1038/pr.2016.206. Epub 2016 Oct 10. Pediatr Res. 2017. PMID: 27723726 Review.
References
-
- Chertow GM, Soroko SH, Paganini EP, et al. Mortality after acute renal failure: models for prognostic stratification and risk adjustment. Kidney Int. 2006;70:1120–1126. - PubMed
-
- Lameire N, Van Biesen W, Vanholder R. Acute renal failure. Lancet. 2005;365:417–430. - PubMed
-
- Uchino S, Kellum JA, Bellomo R, et al. Acute renal failure in critically ill patients: a multinational, multicenter study. JAMA. 2005;294:813–818. - PubMed
-
- Lameire N, Van Biesen W, Vanholder R. Acute kidney injury. Lancet. 2008;372:1863–1865. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
