

Association of residual urine output with mortality, quality of life, and inflammation in incident hemodialysis patients: the Choices for Healthy Outcomes in Caring for End-Stage Renal Disease (CHOICE) Study
- PMID: 20605303
- PMCID: PMC2910835
- DOI: 10.1053/j.ajkd.2010.03.020
Association of residual urine output with mortality, quality of life, and inflammation in incident hemodialysis patients: the Choices for Healthy Outcomes in Caring for End-Stage Renal Disease (CHOICE) Study
Abstract
Background: Residual kidney function (RKF) is associated with improved survival in peritoneal dialysis patients, but its role in hemodialysis patients is less well known. Urine output may provide an estimate of RKF. The aim of our study is to determine the association of urine output with mortality, quality of life (QOL), and inflammation in incident hemodialysis patients.
Study design: Nationally representative prospective cohort study.
Setting & participants: 734 incident hemodialysis participants treated in 81 clinics; enrollment, 1995-1998; follow-up until December 2004.
Predictor: Urine output, defined as producing at least 250 mL (1 cup) of urine daily, ascertained using questionnaires at baseline and year 1.
Outcomes & measurements: Primary outcomes were all-cause and cardiovascular mortality, analyzed using Cox regression adjusted for demographic, clinical, and treatment characteristics. Secondary outcomes were QOL, inflammation (C-reactive protein and interleukin 6 levels), and erythropoietin (EPO) requirements.
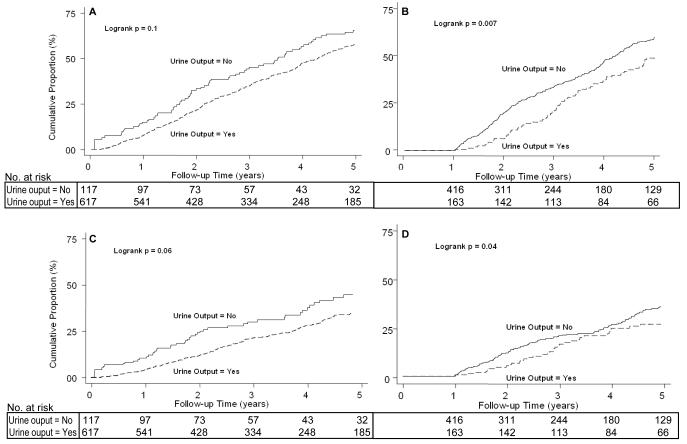
Results: 617 of 734 (84%) participants reported urine output at baseline, and 163 of 579 (28%), at year 1. Baseline urine output was not associated with survival. Urine output at year 1, indicating preserved RKF, was independently associated with lower all-cause mortality (HR, 0.70; 95% CI, 0.52-0.93; P = 0.02) and a trend toward lower cardiovascular mortality (HR, 0.69; 95% CI, 0.45-1.05; P = 0.09). Participants with urine output at baseline reported better QOL and had lower C-reactive protein (P = 0.02) and interleukin 6 (P = 0.03) levels. Importantly, EPO dose was 12,000 U/wk lower in those with urine output at year 1 compared with those without (P = 0.001).
Limitations: Urine volume was measured in only a subset of patients (42%), but agreed with self-report (P < 0.001).
Conclusions: RKF in hemodialysis patients is associated with better survival and QOL, lower inflammation, and significantly less EPO use. RKF should be monitored routinely in hemodialysis patients. The development of methods to assess and preserve RKF is important and may improve dialysis care.
Copyright (c) 2010 National Kidney Foundation, Inc. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Residual kidney function and quality of life in incident hemodialysis patients.Am J Kidney Dis. 2011 Jan;57(1):179; author reply 179-80. doi: 10.1053/j.ajkd.2010.09.020. Am J Kidney Dis. 2011. PMID: 21184925 No abstract available.
References
-
- Perl J, Bargman JM. The importance of residual kidney function for patients on dialysis: a critical review. Am J Kidney Dis. 2009 Jun;53(6):1068–1081. - PubMed
-
- Wang AYM, Lai KN. The importance of residual renal function in dialysis patients. Kidney Int. 2006;69(10):1726–1732. - PubMed
-
- Konings CJ, Kooman JP, Schonck M, et al. Fluid status in CAPD patients is related to peritoneal transport and residual renal function: evidence from a longitudinal study. Nephrol Dial Transplant. 2003 Apr;18(4):797–803. - PubMed
-
- Termorshuizen F, Dekker FW, van Manen JG, Korevaar JC, Boeschoten EW, Krediet RT. Relative contribution of residual renal function and different measures of adequacy to survival in hemodialysis patients: an analysis of the Netherlands Cooperative Study on the Adequacy of Dialysis (NECOSAD)-2. J Am Soc Nephrol. 2004 Apr;15(4):1061–1070. - PubMed
-
- Wang AY-M, Wang M, Woo J, et al. A novel association between residual renal function and left ventricular hypertrophy in peritoneal dialysis patients. Kidney Int. 2002;62(2):639–647. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- K23 DK083514/DK/NIDDK NIH HHS/United States
- K24 DK002643/DK/NIDDK NIH HHS/United States
- R01 DK059616/DK/NIDDK NIH HHS/United States
- 1UO1-DK-57304-01/DK/NIDDK NIH HHS/United States
- K24-DK-02643/DK/NIDDK NIH HHS/United States
- 1 R01 DK070657-01/DK/NIDDK NIH HHS/United States
- U01 DK070657/DK/NIDDK NIH HHS/United States
- R01-DK-59616/DK/NIDDK NIH HHS/United States
- U01 DK057304/DK/NIDDK NIH HHS/United States
- R01 DK080123/DK/NIDDK NIH HHS/United States
- 5T32-DK-007732/DK/NIDDK NIH HHS/United States
- T32 DK007732/DK/NIDDK NIH HHS/United States
- R01-HL-62985/HL/NHLBI NIH HHS/United States
- R01 HL062985/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Research Materials
