

Tight blood pressure control and cardiovascular outcomes among hypertensive patients with diabetes and coronary artery disease
- PMID: 20606150
- PMCID: PMC3008411
- DOI: 10.1001/jama.2010.884
Tight blood pressure control and cardiovascular outcomes among hypertensive patients with diabetes and coronary artery disease
Abstract
Context: Hypertension guidelines advocate treating systolic blood pressure (BP) to less than 130 mm Hg for patients with diabetes mellitus; however, data are lacking for the growing population who also have coronary artery disease (CAD).
Objective: To determine the association of systolic BP control achieved and adverse cardiovascular outcomes in a cohort of patients with diabetes and CAD.
Design, setting, and patients: Observational subgroup analysis of 6400 of the 22,576 participants in the International Verapamil SR-Trandolapril Study (INVEST). For this analysis, participants were at least 50 years old and had diabetes and CAD. Participants were recruited between September 1997 and December 2000 from 862 sites in 14 countries and were followed up through March 2003 with an extended follow-up through August 2008 through the National Death Index for US participants.
Intervention: Patients received first-line treatment of either a calcium antagonist or beta-blocker followed by angiotensin-converting enzyme inhibitor, a diuretic, or both to achieve systolic BP of less than 130 and diastolic BP of less than 85 mm Hg. Patients were categorized as having tight control if they could maintain their systolic BP at less than 130 mm Hg; usual control if it ranged from 130 mm Hg to less than 140 mm Hg; and uncontrolled if it was 140 mm Hg or higher.
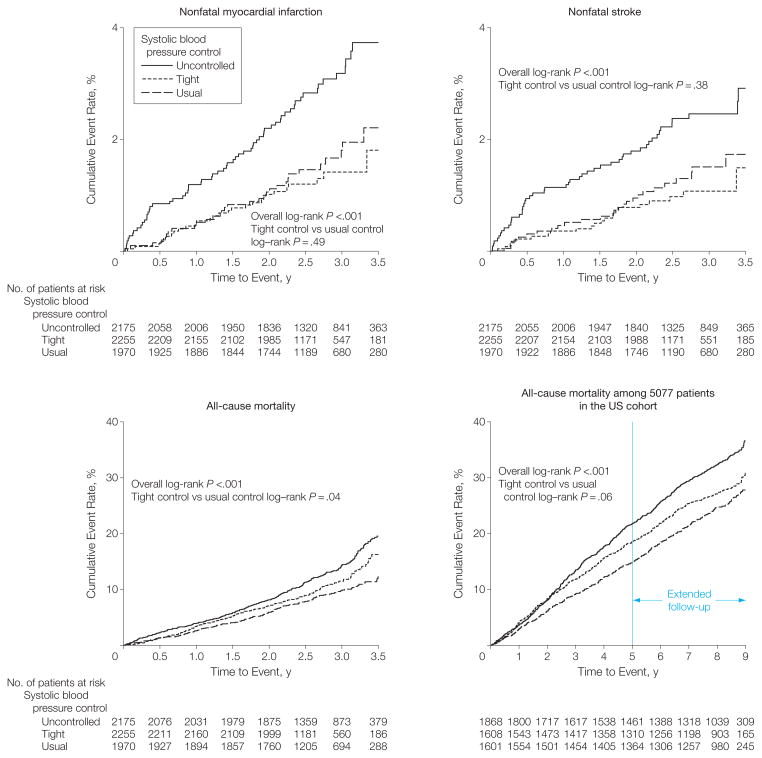
Main outcome measures: Adverse cardiovascular outcomes, including the primary outcomes which was the first occurrence of all-cause death, nonfatal myocardial infarction, or nonfatal stroke.
Results: During 16,893 patient-years of follow-up, 286 patients (12.7%) who maintained tight control, 249 (12.6%) who had usual control, and 431 (19.8%) who had uncontrolled systolic BP experienced a primary outcome event. Patients in the usual-control group had a cardiovascular event rate of 12.6% vs a 19.8% event rate for those in the uncontrolled group (adjusted hazard ratio [HR], 1.46; 95% confidence interval [CI], 1.25-1.71; P < .001). However, little difference existed between those with usual control and those with tight control. Their respective event rates were 12.6% vs 12.7% (adjusted HR, 1.11; 95% CI, 0.93-1.32; P = .24). The all-cause mortality rate was 11.0% in the tight-control group vs 10.2% in the usual-control group (adjusted HR, 1.20; 95% CI, 0.99-1.45; P = .06); however, when extended follow-up was included, risk of all-cause mortality was 22.8% in the tight control vs 21.8% in the usual control group (adjusted HR, 1.15; 95% CI, 1.01-1.32; P = .04).
Conclusion: Tight control of systolic BP among patients with diabetes and CAD was not associated with improved cardiovascular outcomes compared with usual control.
Trial registration: clinicaltrials.gov Identifier: NCT00133692.
Figures


Comment in
-
Hypertension control and cardiovascular outcomes among patients with diabetes and coronary artery disease.JAMA. 2010 Oct 20;304(15):1672; author reply 1672-3. doi: 10.1001/jama.2010.1464. JAMA. 2010. PMID: 20959575 No abstract available.
-
Lowering systolic blood pressure below 130 mm Hg does not improve cardiovascular outcomes in hypertensive patients with diabetes and coronary artery disease.Evid Based Med. 2011 Feb;16(1):24-6. doi: 10.1136/ebm1149. Epub 2010 Nov 3. Evid Based Med. 2011. PMID: 21047847 No abstract available.
References
-
- The 1984 Report of the Joint National Committee on Detection, Evaluation, and Treatment of High Blood Pressure. Arch Intern Med. 1984;144(5):1045–1057. - PubMed
-
- The fifth report of the Joint National Committee on Detection, Evaluation, and Treatment of High Blood Pressure (JNC V) Arch Intern Med. 1993;153(2):154–183. - PubMed
-
- Hansson L, Zanchetti A, Carruthers SG, et al. HOT Study Group. Effects of intensive blood-pressure lowering and low-dose aspirin in patients with hypertension: principal results of the Hypertension Optimal Treatment (HOT) randomised trial. Lancet. 1998;351(9118):1755–1762. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
