

Microalbuminuria: A novel biomarker of sepsis
- PMID: 20606905
- PMCID: PMC2888326
- DOI: 10.4103/0972-5229.63034
Microalbuminuria: A novel biomarker of sepsis
Abstract
Context: Diffused endothelial dysfunction in sepsis leads to an increase in systemic capillary permeability, the renal component manifesting as microalbuminuria. The degree of microalbuminuria correlates with the severity of the acute insult, the quantification of which may serve to predict sepsis and mortality in critically ill patients.
Aims: To evaluate whether the degree of microalbuminuria could differentiate patients with sepsis from those without and predict mortality in critically ill patients.
Settings and design: Prospective, non-interventional study in a 20-bed Intensive Care Unit (ICU) of a tertiary care hospital.
Methods and materials: After exclusions, between Jan-May 2007, 94 consecutive adult patients were found eligible. Albumin-creatinine ratio (ACR, mg/g) was measured in urine samples collected on ICU admission (ACR1) and at 24 hours (ACR2).
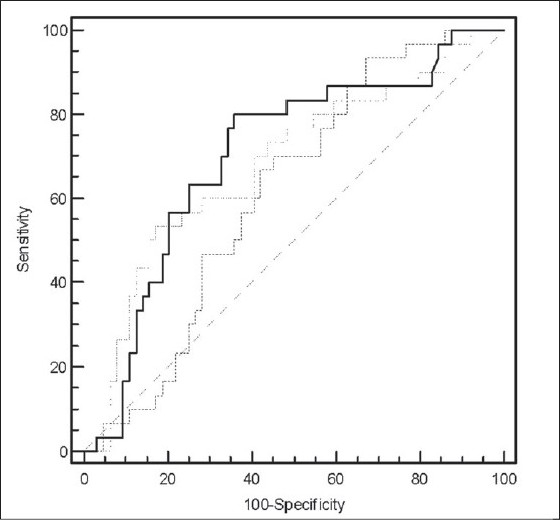
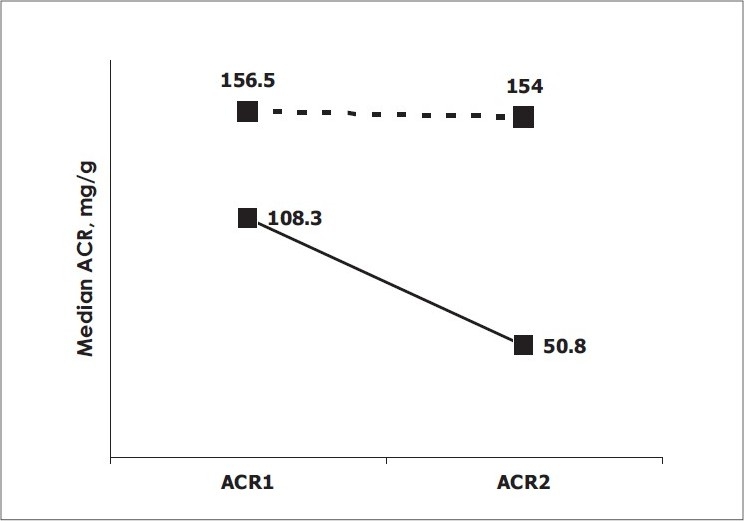
Results: PATIENTS WERE CLASSIFIED INTO TWO GROUPS: those with sepsis, severe sepsis and septic shock (n = 30) and those without sepsis [patients without systemic inflammatory response syndrome (SIRS) and with SIRS due to noninfectious causes] (n = 64). In the sepsis group, median ACR1 [206.5 (IQR129.7-506.1)] was significantly higher compared to the non sepsis group [76.4 (IQR29-167.1)] (P = 0.0016, Mann Whitney). The receiver operating characteristics (ROC) curve analysis showed that at a cut off value 124 mg/g, ACR1 may be able to discriminate between patients with and without sepsis with a sensitivity of 80%, specificity of 64.1%, positive predictive value (PPV) of 51.1% and negative predictive value (NPV) of 87.3%. The median ACR2 [154 (IQR114.4-395.3)] was significantly higher (P = 0.004) in nonsurvivors (n = 13) as compared to survivors [50.8 (IQR 21.6-144.7)]. The ROC curve analysis revealed that ACR2 at a cut-off of 99.6 mg/g could predict ICU mortality with sensitivity of 85%, specificity of 68% with a NPV of 97% and PPV of 30%.
Conclusion: Absence of significant microalbuminuria on ICU admission is unlikely to be associated with sepsis. At 24 hours, absence of elevated levels of microalbuminuria is strongly predictive of ICU survival, equivalent to the time-tested APACHE II scores.
Keywords: Capillary permeability; critically ill; intensive care units; microalbuminuria; mortality; sepsis.
Conflict of interest statement
Figures

References
-
- Angus DC, Linde-Zwirble WT, Lidicker J. Epidemiology of severe sepsis in the United States: Analysis of incidence, outcome, and associated costs of care. Crit Care Med. 2001;29:1303–10. - PubMed
-
- Todi S, Chatterjee S, Bhattacharyya M. Epidemiology of severe sepsis in India. Crit Care. 2007;11:65.
-
- Rivers E, Nguyen B, Havstad S, Ressler J, Muzzin A, Knoblich B, et al. Early goal-directed therapy in the treatment of severe sepsis and septic shock. N Engl J Med. 2001;345:1368–77. - PubMed
-
- Wheeler AP, Steingrub J, Linde-Zwirble W, McCollam JS, Zeckel M. Prompt administration of drotrecogin alfa (activated) is associated with improved survival. Crit Care Med. 2003;12:A120.
-
- Hotchkiss RS, Karl IE. The pathophysiology and treatment of sepsis. N Engl J Med. 2003;348:138–50. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous