

2D-fluoroscopic navigated percutaneous screw fixation of pelvic ring injuries--a case series
- PMID: 20609243
- PMCID: PMC2916892
- DOI: 10.1186/1471-2474-11-153
2D-fluoroscopic navigated percutaneous screw fixation of pelvic ring injuries--a case series
Abstract
Background: Screw fixation of pelvic ring fractures is a common, but demanding procedure and navigation techniques were introduced to increase the precision of screw placement. The purpose of this case series was the evaluation of screw misplacement rate and functional outcome of percutaneous screw fixation of pelvic ring disruptions using a 2D navigation system.
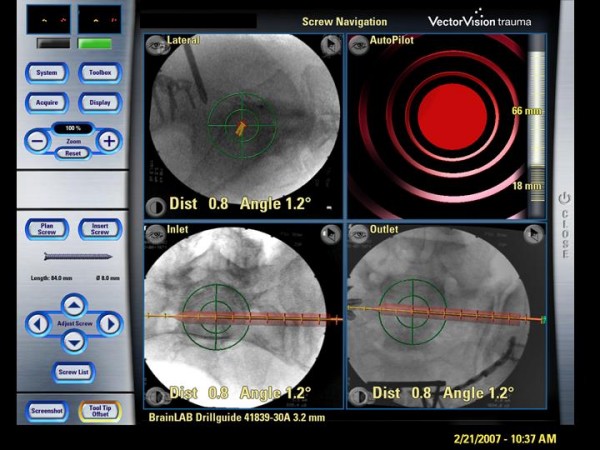
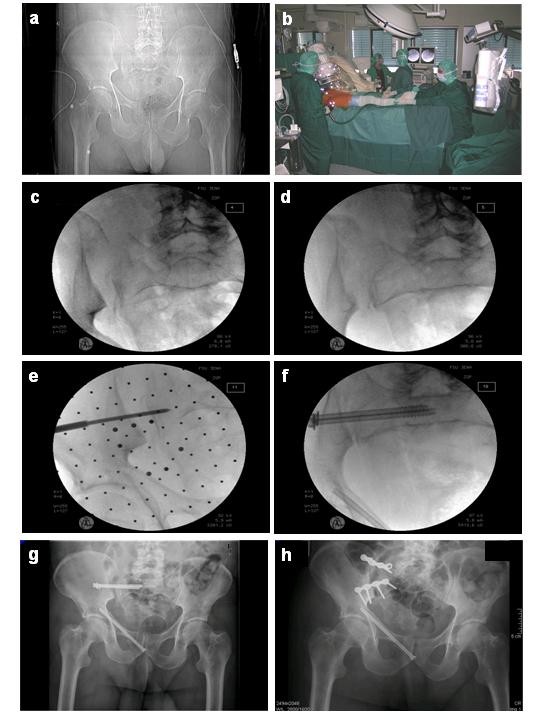
Methods: Between August 2004 and December 2007, 44 of 442 patients with pelvic injuries were included for closed reduction and percutaneous screw fixation of disrupted pelvic ring lesions using an optoelectronic 2D-fluoroscopic based navigation system. Operating and fluoroscopy time were measured, as well as peri- and postoperative complications documented. Screw position was assessed by postoperative CT scans. Quality of live was evaluated by SF 36-questionnaire in 40 of 44 patients at mean follow up 15.5 +/- 1.2 month.
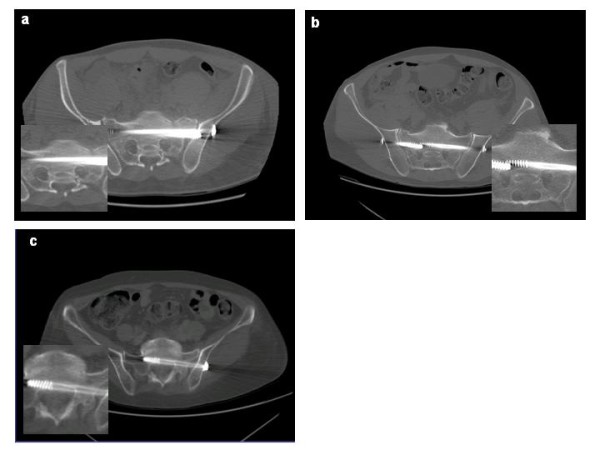
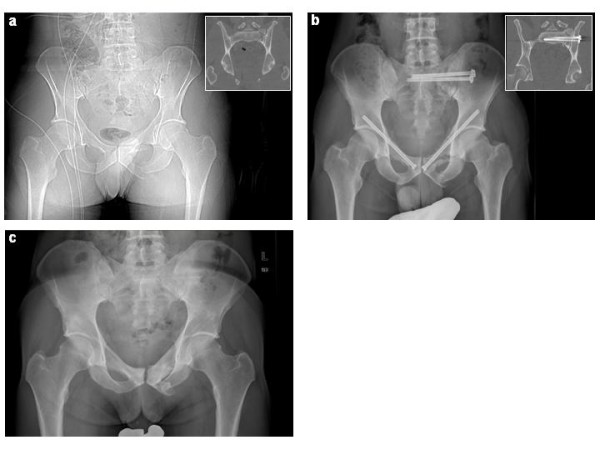
Results: 56 iliosacral- and 29 ramus pubic-screws were inserted (mean operation time per screw 62 +/- 4 minutes, mean fluoroscopy time per screw 123 +/- 12 seconds). In post-operative CT-scans the screw position was assessed and graded as follows: I. secure positioning, completely in the cancellous bone (80%); II. secure positioning, but contacting cortical bone structures (14%); III. malplaced positioning, penetrating the cortical bone (6%). The malplacements predominantly occurred in bilateral overlapping screw fixation. No wound infection or iatrogenic neurovascular damage were observed. Four re-operations were performed, two of them due to implant-misplacement and two of them due to implant-failure.
Conclusion: 2D-fluoroscopic navigation is a safe tool providing high accuracy of percutaneous screw placement for pelvic ring fractures, but in cases of a bilateral iliosacral screw fixation an increased risk for screw misplacement was observed. If additional ramus pubic screw fixations are performed, the retrograde inserted screws have to pass the iliopubic eminence to prevent an axial screw loosening.
Figures
References
-
- Matta JM, Saucedo T. Internal fixation of pelvic ring fractures. Clin Orthop Relat Res. 1989. pp. 83–97. - PubMed
-
- Fuchtmeier B, Maghsudi M, Neumann C, Hente R, Roll C, Nerlich M. The minimally invasive stabilization of the dorsal pelvic ring with the transiliacal internal fixator (TIFI)--surgical technique and first clinical findings. Unfallchirurg. 2004;107:1142–1151. doi: 10.1007/s00113-004-0824-9. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
