

Safety of aprotinin in congenital heart operations: results from a large multicenter database
- PMID: 20609740
- PMCID: PMC3263763
- DOI: 10.1016/j.athoracsur.2010.02.073
Safety of aprotinin in congenital heart operations: results from a large multicenter database
Abstract
Background: Aprotinin was used frequently in children undergoing congenital heart operations with the aim of reducing bleeding, until it was taken off the market after adult studies reported increased renal failure and death. We evaluated the safety of aprotinin in a large multicenter cohort of children undergoing congenital heart operations.
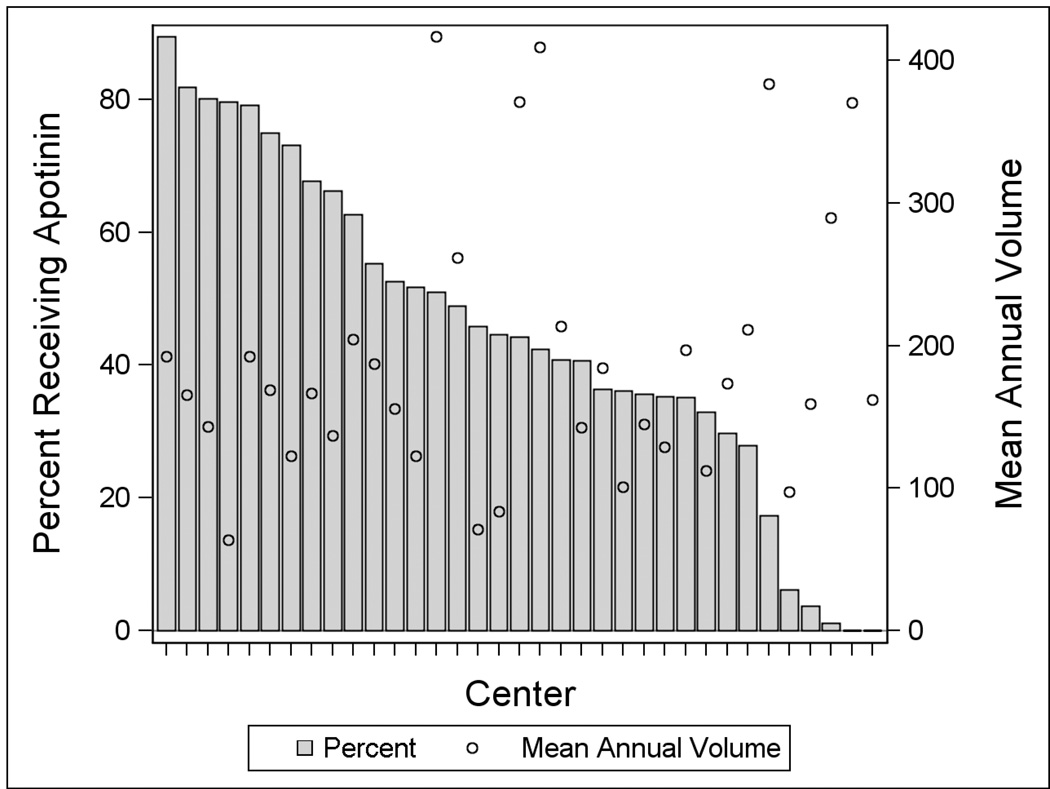
Methods: The Pediatric Health Information Systems Database was used to evaluate aprotinin in children (aged 0 to 18 years) undergoing congenital heart operations at 35 children's hospitals from 2003 to 2007. Propensity scores were constructed to account for potential confounders of age, sex, race, prematurity, genetic syndrome, type of operation (Risk Adjustment in Congenital Heart Surgery-1 category), center, and center volume. Multivariable analysis, adjusting for propensity score and individual covariates was performed to evaluate in-hospital mortality, postoperative renal failure requiring dialysis, and length of stay. Subanalysis was performed in the high-risk cohort undergoing reoperation.
Results: The study included 30,372 patients (56% male) who were a median age of 7 months (interquartile range, 36 days to 3.2 years). Overall, 44% received aprotinin. Multivariable analysis found no difference in postoperative mortality (odds ratio, 1.00; 95% confidence interval [CI], 0.99 to 1.01), dialysis (odds ratio, 1.00; 95% CI, 0.99 to 1.01), or length of stay (least square mean difference, -0.44 days; 95% CI, -1.01 to 0.13) between aprotinin recipients and nonrecipients. No difference was found in mortality or dialysis in patients undergoing reoperation. Aprotinin recipients in the reoperation subgroup had significantly reduced length of stay (least square mean difference, -2.05 days; 95% CI -3.29 to -0.81),
Conclusions: These data suggest aprotinin is not associated with increased mortality or dialysis in children undergoing congenital heart operations and that further evaluation of aprotinin in this population could be undertaken without undue risk.
Copyright 2010 The Society of Thoracic Surgeons. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Can we really believe that aprotinin is safe in congenital heart surgery?Ann Thorac Surg. 2011 Mar;91(3):987-8; author reply 988. doi: 10.1016/j.athoracsur.2010.07.106. Ann Thorac Surg. 2011. PMID: 21353050 No abstract available.
References
-
- Arnold DM, Fergusson DA, Chan AK, et al. Avoiding transfusions in children undergoing cardiac surgery: A meta-analysis of randomized trials of aprotinin. Anesth Analg. 2006;102:731–737. - PubMed
-
- Sedrakyan A, Treasure T, Elefteriades JA. Effect of aprotinin on clinical outcomes in coronary artery bypass graft surgery: a systematic review and meta-analysis of randomized clinical trials. J Thorac Cardiovasc Surg. 2004;128:442–448. - PubMed
-
- Tassani P, Augustin N, Barankay A, Braun SL, Zaccaria F, Richter JA. High dose aprotinin modulates the balance between proinflammatory and anti-inflammatory response during coronary artery bypass graft surgery. J Cardiovasc Thorac Surg. 2000;14:682–686. - PubMed
-
- Hill GE, Alonso A, Spurzem JR, et al. Aprotinin and methylprednisolone equally blunt cardiopulmonary bypass-induced inflammation in humans. J Thorac Cardiovasc Surg. 1995;110:1658–1662. - PubMed
-
- Fergusson DA, Hebert PC, Mazer CD, et al. A comparison of aprotinin and lysine analgues in high-risk cardiac surgery. N Engl J Med. 2008;358:2319–2331. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
