

Low energy diet and intracranial pressure in women with idiopathic intracranial hypertension: prospective cohort study
- PMID: 20610512
- PMCID: PMC2898925
- DOI: 10.1136/bmj.c2701
Low energy diet and intracranial pressure in women with idiopathic intracranial hypertension: prospective cohort study
Abstract
Objective: To observe intracranial pressure in women with idiopathic intracranial hypertension who follow a low energy diet.
Design: Prospective cohort study.
Setting: Outpatient department and the clinical research facility based at two separate hospitals within the United Kingdom.
Participants: 25 women with body mass index (BMI) >25, with active (papilloedema and intracranial pressure >25 cm H(2)O), chronic (over three months) idiopathic intracranial hypertension. Women who had undergone surgery to treat idiopathic intracranial hypertension were excluded.
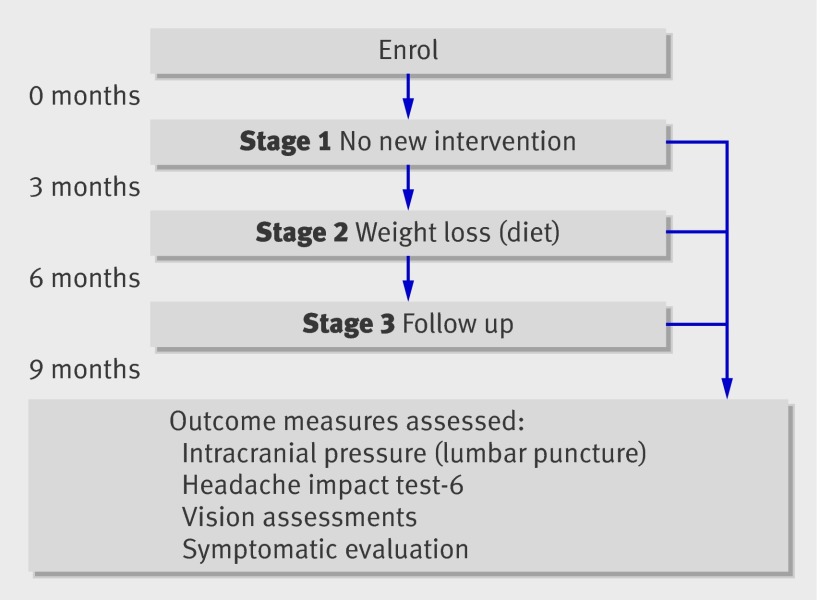
Intervention: Stage 1: no new intervention; stage 2: nutritionally complete low energy (calorie) diet (1777 kJ/day (425 kcal/day)); stage 3: follow-up period after the diet. Each stage lasted three months.
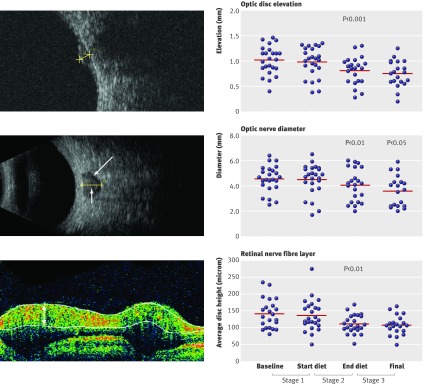
Main outcome measure: The primary outcome was reduction in intracranial pressure after the diet. Secondary measures included score on headache impact test-6, papilloedema (as measured by ultrasonography of the elevation of the optic disc and diameter of the nerve sheath, together with thickness of the peripapillary retina measured by optical coherence tomography), mean deviation of Humphrey visual field, LogMAR visual acuity, and symptoms. Outcome measures were assessed at baseline and three, six, and nine months. Lumbar puncture, to quantify intracranial pressure, was measured at baseline and three and six months.
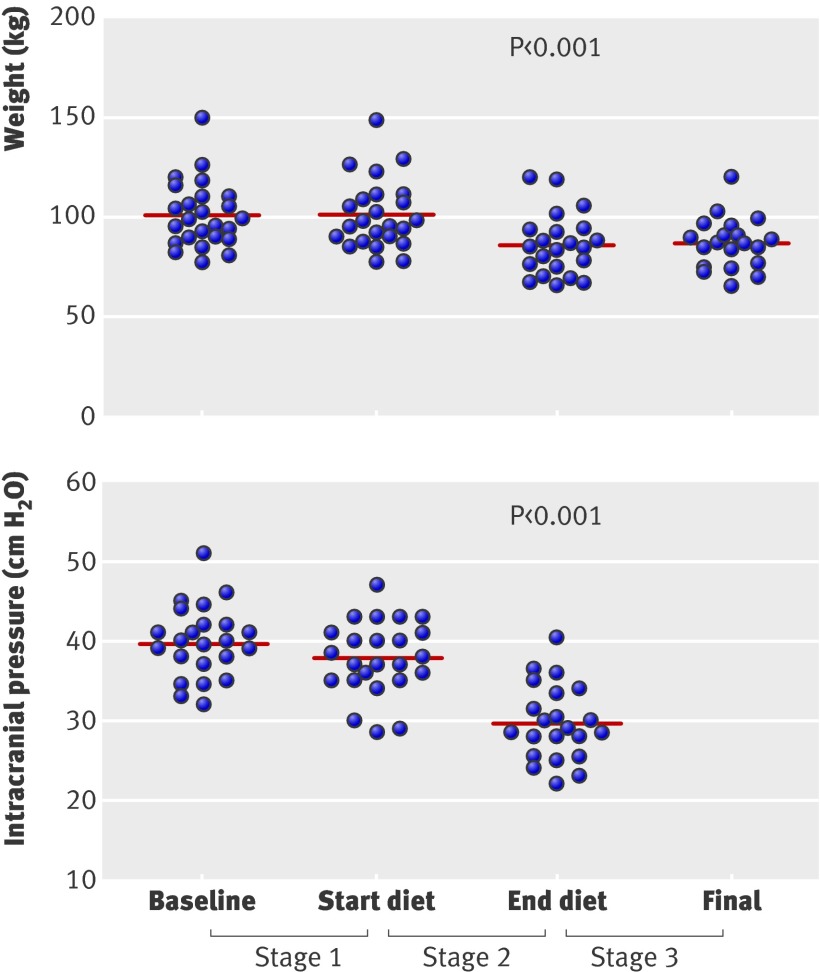
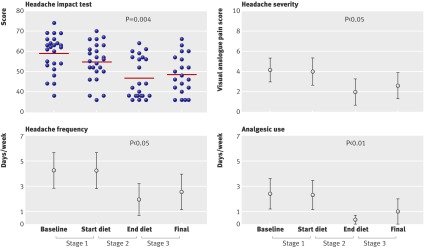
Results: All variables remained stable over stage 1. During stage 2, there were significant reductions in weight (mean 15.7 (SD 8.0) kg, P<0.001), intracranial pressure (mean 8.0 (SD 4.2) cm H(2)O, P<0.001), score on headache impact test (7.6 (SD 10.1), P=0.004), and papilloedema (optic disc elevation (mean 0.15 (SD 0.23) mm, P=0.002), diameter of the nerve sheath (mean 0.7 (SD 0.8) mm, P=0.004), and thickness of the peripapillary retina (mean 25.7 (SD 36.1) micro, P=0.001)). Mean deviation of the Humphrey visual field remained stable, and in only five patients, the LogMAR visual acuity improved by one line. Fewer women reported symptoms including tinnitus, diplopia, and obscurations (10 v 4, P=0.004; 7 v 0, P=0.008; and 4 v 0, P=0.025, respectively). Re-evaluation at three months after the diet showed no significant change in weight (0.21 (SD 6.8) kg), and all outcome measures were maintained.
Conclusion: Women with idiopathic intracranial hypertension who followed a low energy diet for three months had significantly reduced intracranial pressure compared with pressure measured in the three months before the diet, as well as improved symptoms and reduced papilloedema. These reductions persisted for three months after they stopped the diet.
Conflict of interest statement
Competing interests: All authors have completed the Unified Competing Interest form at
Figures
Comment in
-
Idiopathic intracranial hypertension.BMJ. 2010 Jul 7;341:c2836. doi: 10.1136/bmj.c2836. BMJ. 2010. PMID: 20610513 No abstract available.
References
-
- Sinclair AJ, Ball AK, Burdon MA, Clarke CE, Stewart PM, Curnow SJ, et al. Exploring the pathogenesis of IIH: an inflammatory perspective. J Neuroimmunol 2008;201-2:212-20. - PubMed
-
- Corbett JJ, Savino PJ, Thompson HS, Kansu T, Schatz NJ, Orr LS, et al. Visual loss in pseudotumor cerebri. Follow-up of 57 patients from five to 41 years and a profile of 14 patients with permanent severe visual loss. Arch Neurol 1982;39:461-74. - PubMed
-
- WHO. Global database on body mass index. 2010. http://apps.who.int/bmi/index.jsp.
-
- Lueck C, McIlwaine G. Interventions for idiopathic intracranial hypertension. Cochrane Database Syst Rev 2005;3:CD003434. - PubMed
-
- Glueck CJ, Aregawi D, Goldenberg N, Golnik KC, Sieve L, Wang P. Idiopathic intracranial hypertension, polycystic-ovary syndrome, and thrombophilia. J Lab Clin Med 2005;145:72-82. - PubMed