

Histologic identification of human papillomavirus (HPV)-related squamous cell carcinoma in cervical lymph nodes: a reliable predictor of the site of an occult head and neck primary carcinoma
- PMID: 20614311
- PMCID: PMC2807564
- DOI: 10.1007/s12105-008-0066-1
Histologic identification of human papillomavirus (HPV)-related squamous cell carcinoma in cervical lymph nodes: a reliable predictor of the site of an occult head and neck primary carcinoma
Abstract
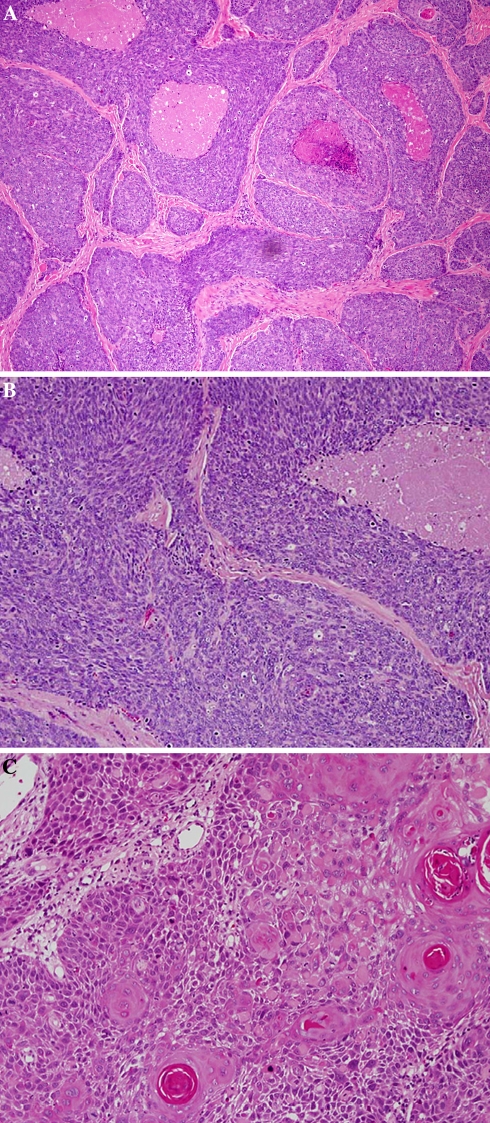
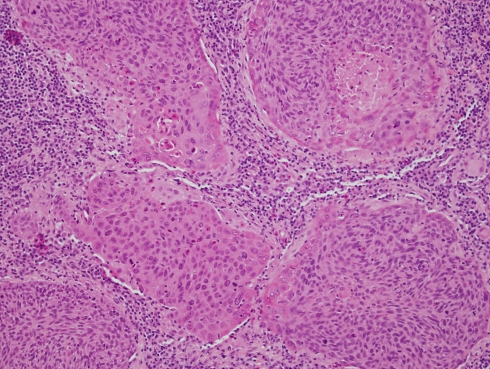
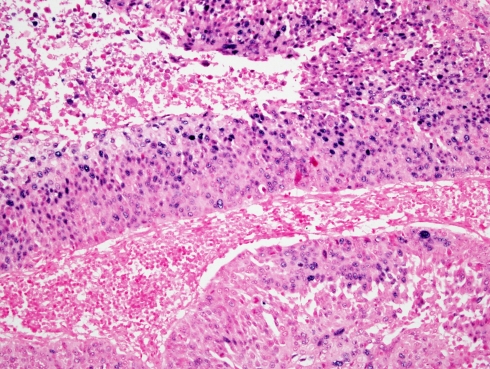
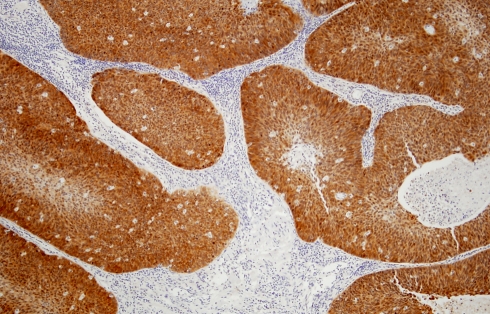
Objective: Patients with head and neck squamous cell carcinoma (SCC) often present with cervical lymph node metastasis. Occasionally the primary tumor site remains unknown even after thorough investigation. Management of such cases is problematic and may result in over-treatment and consequent increased morbidity. High risk HPV has been advocated recently as an important etiologic factor for a subset of head and neck SCC. These are believed to have a special predilection for the oropharyngeal tonsils and are characterized by nonkeratinizing basaloid morphology, and a strong reactivity to p16 immunostain. Identifying HPV-related SCC in the lymph nodes may thus provide a means for localizing the primary tumor site.
Design: Ninety-three cases of SCC metastatic to the neck from known primary tumors were classified morphologically into conventional keratinizing SCC (KSCC) and non-keratinizing SCC (NKCa). In situ hybridization (ISH) for high risk HPV as well as immunostaining for p16 were performed on all metastsatic and primary tumors.
Results: Of the 93 cases of metastatic carcinomas 32 were oropharyngeal, 35 oral, and 26 arose in the laryx/hypopharynx. Twenty-three cases were found to be HPV+ by ISH, of which 22/23 had oropharyngeal origin (P < 0.0001), with 95.7% sensitivity and 85.7% specificity. Twenty-one of these HPV+ oropharyngeal tumors were NKCa (P < 0.0001). The remaining case showed overlapping NKCa/KSCC hybrid morphology. All NKCa were HPV+ and stained diffusely and strongly with p16 antibodies.
Conclusion: We have demonstrated that HPV status of the lymph node metastasis can be assessed not only by ISH and p16 immunoreactivity but also histomorphologically. In addition, a positive microscopic identification of HPV-related carcinoma is a reliable predictor of oropharyngeal origin.
Keywords: HPV; ISH; Nonkeratinizing squamous cell carcinoma; Occult head and neck carcinoma; Oropharynx; p16.
Figures
Similar articles
-
Detection of human papillomavirus-related squamous cell carcinoma cytologically and by in situ hybridization in fine-needle aspiration biopsies of cervical metastasis: a tool for identifying the site of an occult head and neck primary.Cancer. 2008 Apr 25;114(2):118-23. doi: 10.1002/cncr.23348. Cancer. 2008. PMID: 18300234
-
Adenosquamous carcinoma of the head and neck: relationship to human papillomavirus and review of the literature.Head Neck Pathol. 2011 Jun;5(2):108-16. doi: 10.1007/s12105-011-0245-3. Epub 2011 Feb 9. Head Neck Pathol. 2011. PMID: 21305368 Free PMC article. Review.
-
Squamous cell carcinoma metastatic to neck from an unknown primary: the potential impact of modern pathologic evaluation on perceived incidence of human papillomavirus-positive oropharyngeal carcinoma prior to 1970.Laryngoscope. 2012 Apr;122(4):793-6. doi: 10.1002/lary.21899. Epub 2012 Jan 17. Laryngoscope. 2012. PMID: 22252715
-
Fine-needle aspiration of cervical lymph nodes yields adequate materials for accurate HPV testing in metastatic head and neck squamous cell carcinomas.Diagn Cytopathol. 2016 Oct;44(10):792-8. doi: 10.1002/dc.23548. Epub 2016 Jul 28. Diagn Cytopathol. 2016. PMID: 27465660
-
Synchronous bilateral tonsillar squamous cell carcinoma related to human papillomavirus: Two case reports and a brief review of the literature.Ear Nose Throat J. 2016 Apr-May;95(4-5):E30-4. Ear Nose Throat J. 2016. PMID: 27140027 Review.
Cited by
-
Using Texture Analysis to Determine Human Papillomavirus Status of Oropharyngeal Squamous Cell Carcinomas on CT.AJNR Am J Neuroradiol. 2015 Jul;36(7):1343-8. doi: 10.3174/ajnr.A4285. Epub 2015 Apr 2. AJNR Am J Neuroradiol. 2015. PMID: 25836725 Free PMC article.
-
Detection of HPV infection in head and neck squamous cell carcinoma: a practical proposal.Virchows Arch. 2013 Apr;462(4):381-9. doi: 10.1007/s00428-013-1393-5. Epub 2013 Mar 17. Virchows Arch. 2013. PMID: 23503925
-
Small lymphocytic lymphoma obscuring microscopic tonsillar squamous cell carcinoma: an unknown occurrence with a known primary.Head Neck Pathol. 2012 Mar;6(1):125-9. doi: 10.1007/s12105-010-0228-9. Epub 2010 Dec 1. Head Neck Pathol. 2012. PMID: 21120710 Free PMC article.
-
Review: Head and neck squamous cell carcinoma in sub-Saharan Africa.Malawi Med J. 2015 Sep;27(3):79-87. doi: 10.4314/mmj.v27i3.2. Malawi Med J. 2015. PMID: 26715951 Free PMC article. Review.
-
Management of neck metastases of unknown primary origin united in two European centers.Eur Arch Otorhinolaryngol. 2015 Jan;272(1):195-205. doi: 10.1007/s00405-014-2934-5. Epub 2014 Mar 11. Eur Arch Otorhinolaryngol. 2015. PMID: 24615648
References
-
- Braud F, al-Sarraf M. Diagnosis and management of squamous cell carcinoma of unknown primary tumor site of the neck. Semin Oncol. 1993;20:273–8. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
