

Benign fibro-osseous lesions of the craniofacial complex. A review
- PMID: 20614314
- PMCID: PMC2807558
- DOI: 10.1007/s12105-008-0057-2
Benign fibro-osseous lesions of the craniofacial complex. A review
Abstract
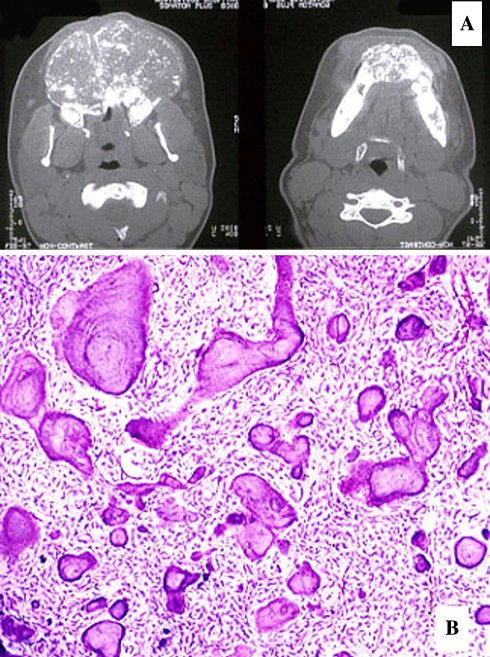
Benign fibro-osseous lesions of the craniofacial complex are represented by a variety of disease processes that are characterized by pathologic ossifications and calcifications in association with a hypercellular fibroblastic marrow element. The current classification includes neoplasms, developmental dysplastic lesions and inflammatory/reactive processes. The definitive diagnosis can rarely be rendered on the basis of histopathologic features alone; rather, procurement of a final diagnosis is usually dependent upon assessment of microscopic, clinical and imaging features together. Fibrous dysplasia and osteitis deformans constitute two dysplastic lesions in which mutations have been uncovered. Other dysplastic bone diseases of the craniofacial complex include florid osseous dysplasia, focal cemento-osseous dysplasia and periapical cemental dysplasia, all showing a predilection for African descent individuals; although no specific genetic alterations in DNA coding have yet to be uncovered and most studies have been derived from predominant high African descent populations. Ossifying fibromas are neoplastic lesions with four subtypes varying with regard to behavior and propensity for recurrence after surgical excision. The clinicopathologic and molecular features of this unique yet heterogeneous group of diseases are reviewed.
Keywords: Benign fibroosseous lesions; Cementoma; Cementoosseous dysplasia; Fibrous dysplasia; Ossifying fibroma; Osteitis deformans.
Figures
References
-
- Waldron CA, Giansanti JS, Browand BC. Sclerotic cemental masses of the jaws (so-called chronic sclerosing osteomyelitis, sclerosing osteitis, multiple enostosis, and gigantiform cementoma. Oral Surg Oral Med Oral Pathol. 1975;39:590–604. - PubMed
-
- Waldron CA, Giansanti JS. Benign fibro-osseous lesions of the jaws: a clinical-radiologic-histologic review of sixty-five cases. Oral Surg Oral Med Oral Pathol. 1973;35:190–201. - PubMed
-
- Waldron CA, Giansanti JS. Benign fibro-osseous lesions of the jaws: a clinical-radiologic-histologic review of sixty-five cases. II. Benign fibro-osseous lesions of periodontal ligament origin. Oral Surg Oral Med Oral Pathol. 1973;35:340–50. - PubMed
-
- Hamner JE, 3rd, Scofield HH, Cornyn J. Benign fibro-osseous jaw lesions of periodontal membrane origin. An analysis of 249 cases. Cancer. 1968;22:861–78. - PubMed
-
- Eversole LR, Sabes WR, Rovin S. Fibrous dysplasia: a nosologic problem in the diagnosis of fibro-osseous lesions of the jaws. J Oral Pathol. 1972;1:189–220. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
