

Hospitalisation and bed rest for multiple pregnancy
- PMID: 20614420
- PMCID: PMC7051031
- DOI: 10.1002/14651858.CD000110.pub2
Hospitalisation and bed rest for multiple pregnancy
Abstract
Background: Bed rest used to be widely advised for women with a multiple pregnancy.
Objectives: The objective was to assess the effect of bed rest in hospital for women with a multiple pregnancy for prevention of preterm birth and other fetal, neonatal and maternal outcomes.
Search strategy: We searched the Cochrane Pregnancy and Childbirth Group's Trials Register (May 2010).
Selection criteria: Randomised trials which compare outcomes in women with a multiple pregnancy and their babies who were offered bed rest in hospital with women only admitted to hospital if complications occurred.
Data collection and analysis: The review authors carried out assessment for inclusion and risk of bias of the trials. We extracted and double entered data, and used a random-effects model.
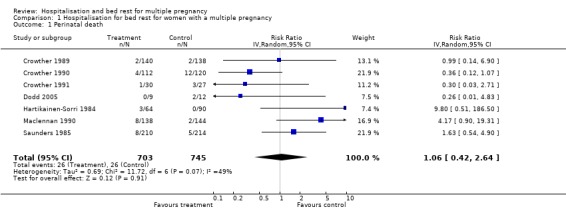
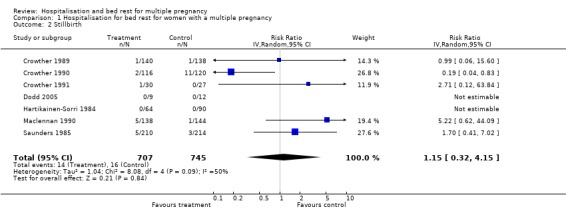
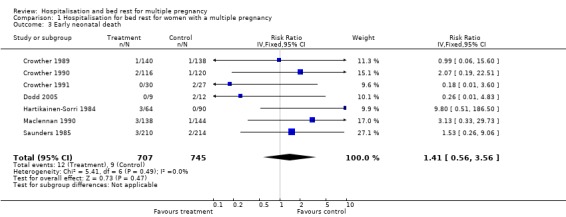
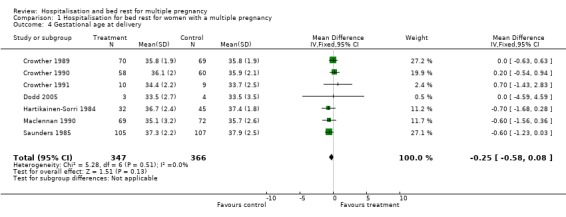
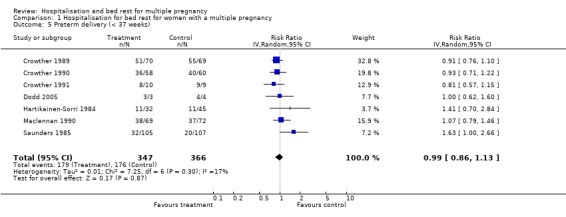
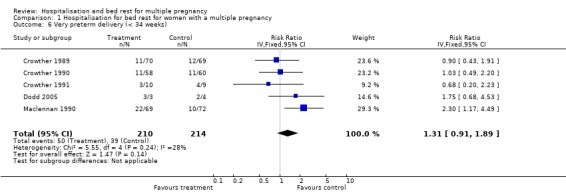
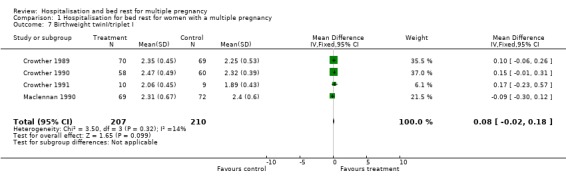
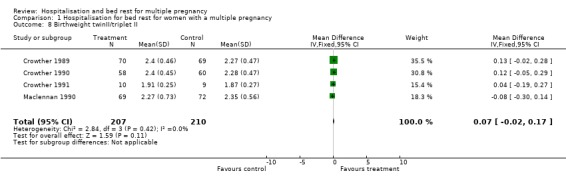
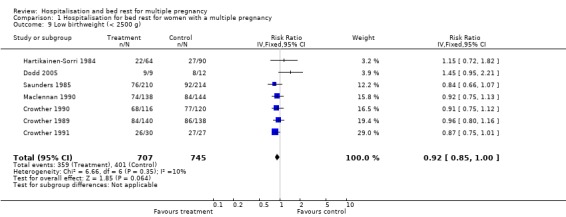
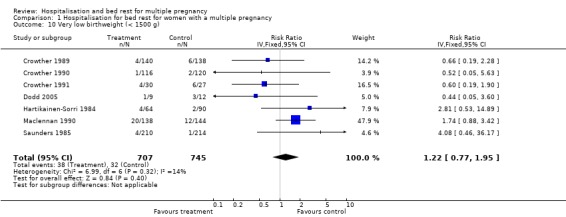
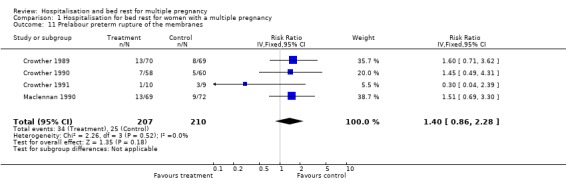
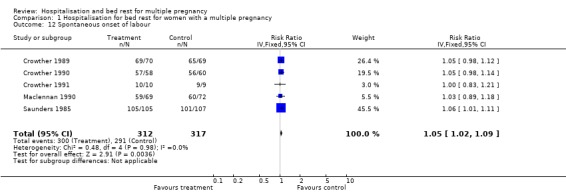
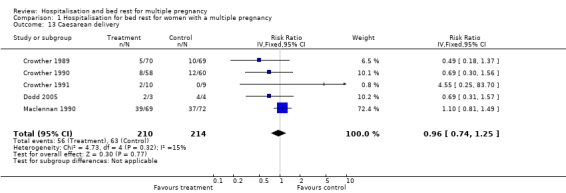
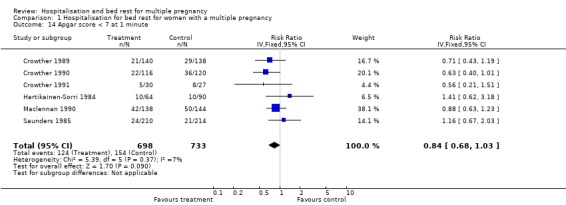
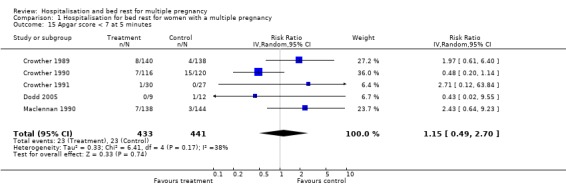
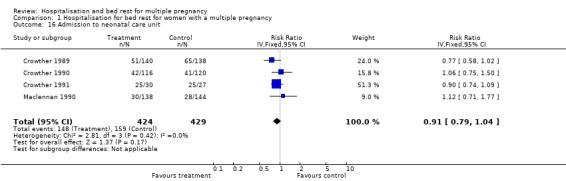
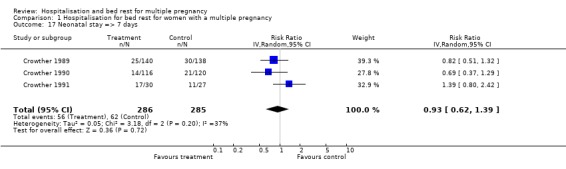
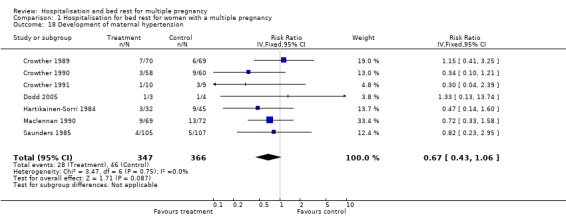
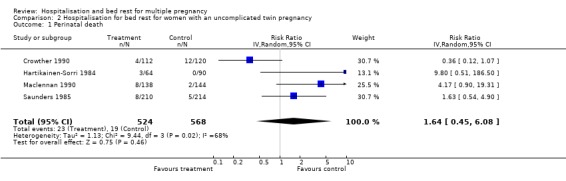
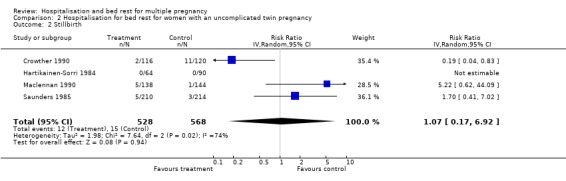
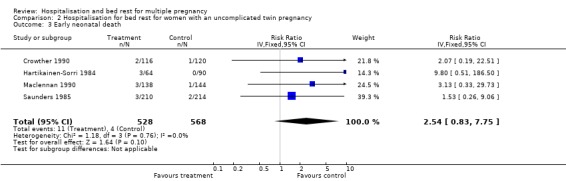
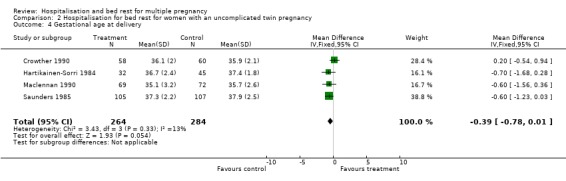
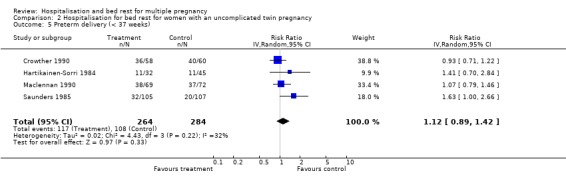
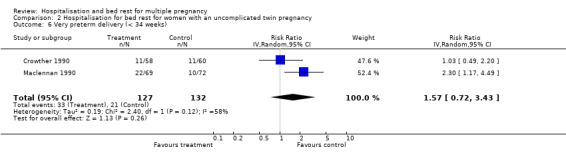
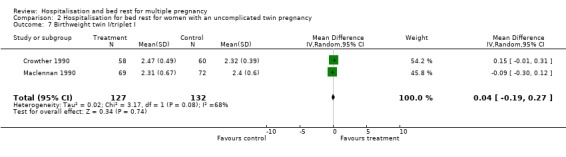
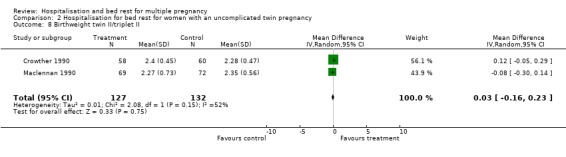
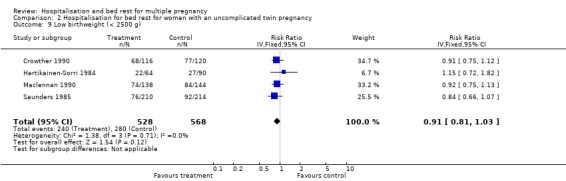
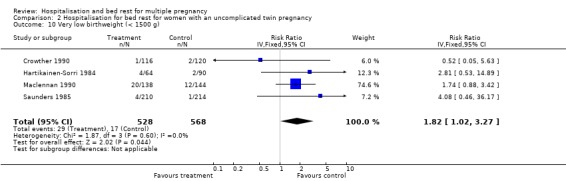
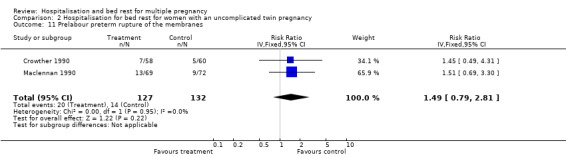
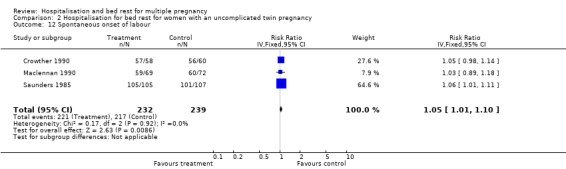
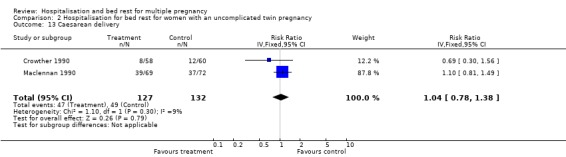
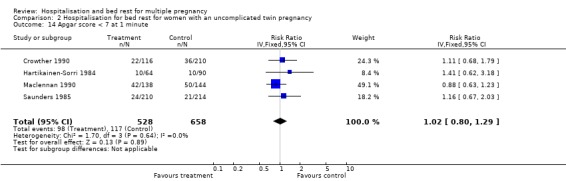
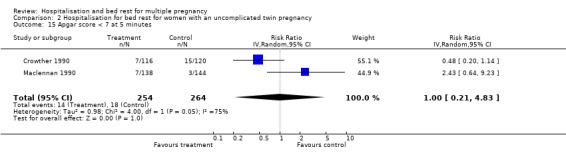
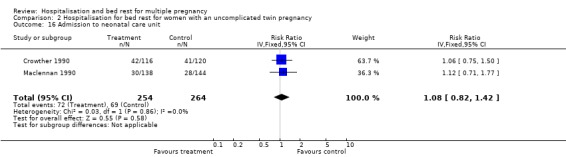
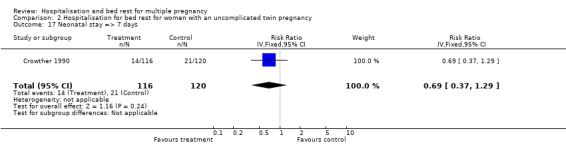
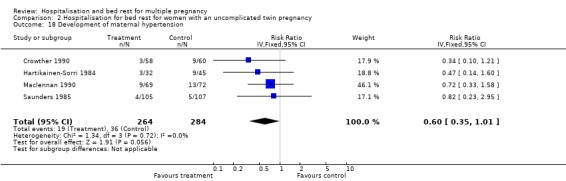
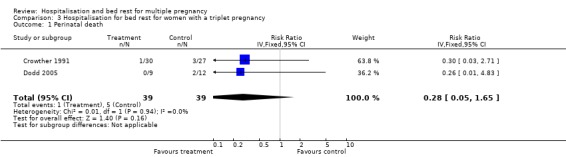
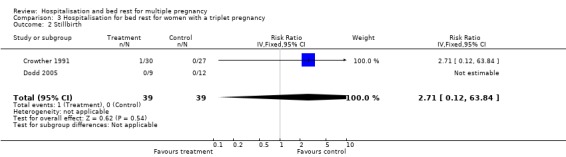
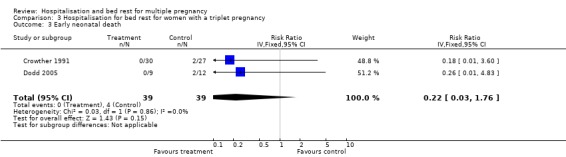
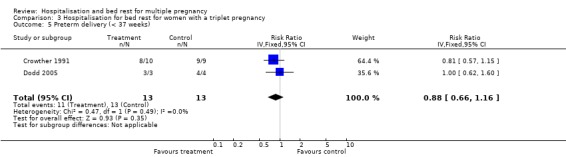
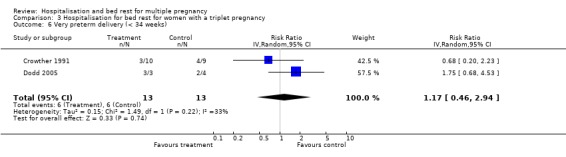
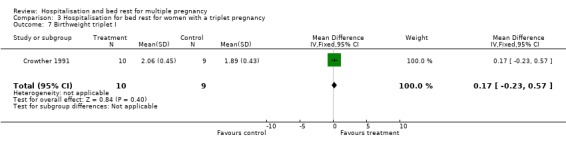
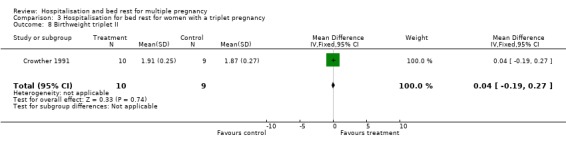
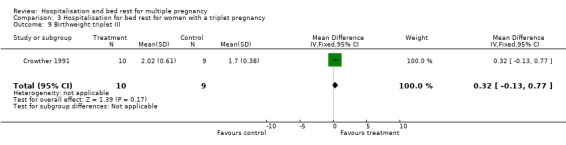
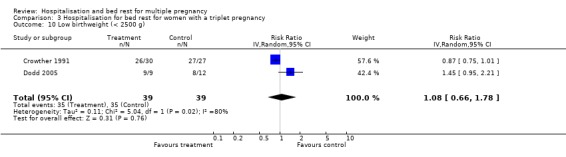
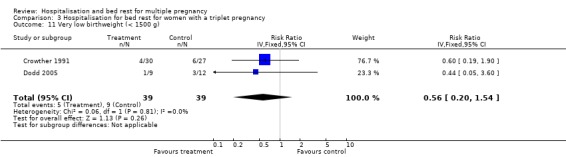
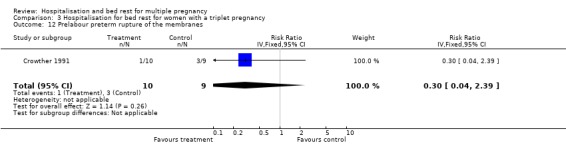
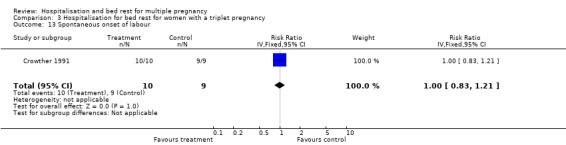
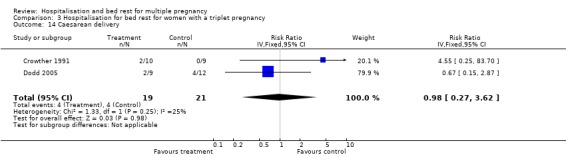
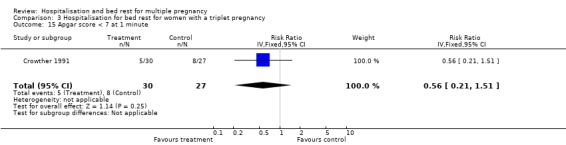
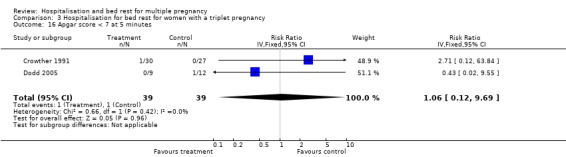
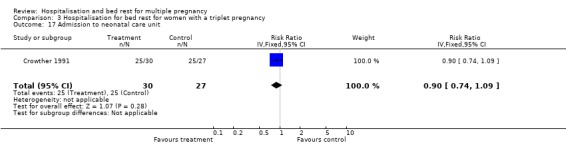
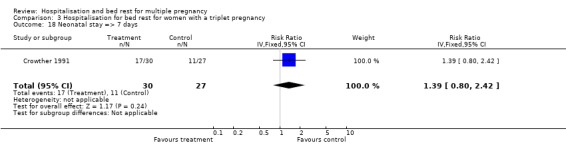
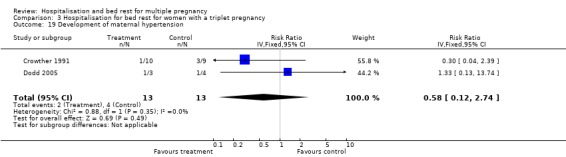
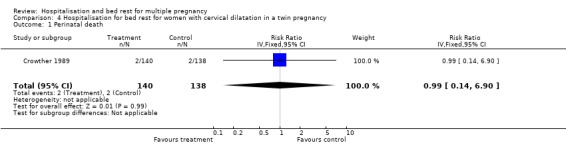
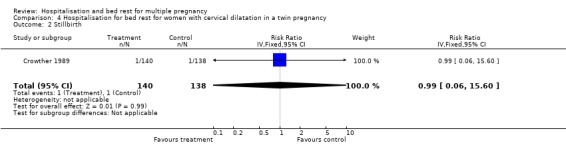
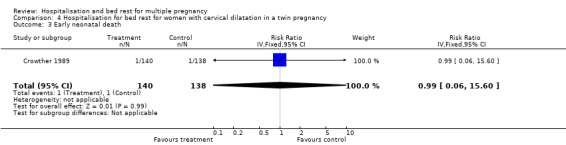
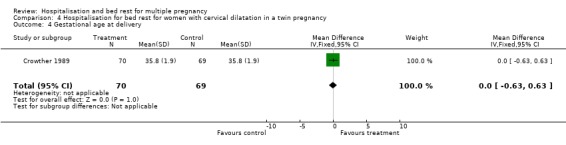
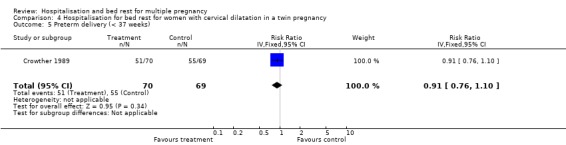
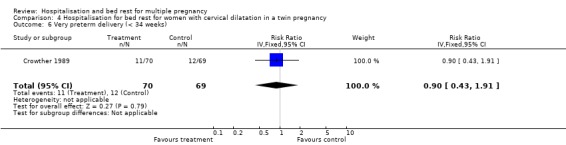
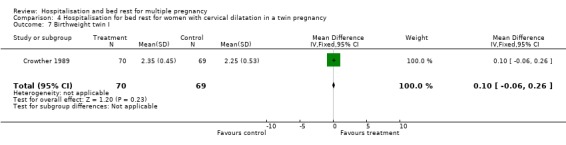
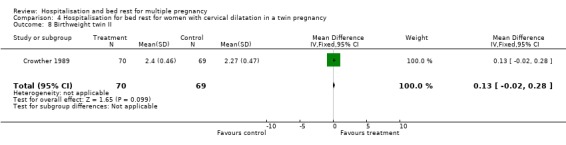
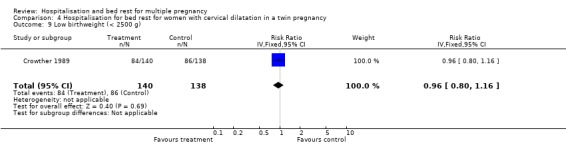
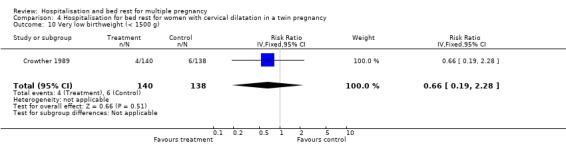
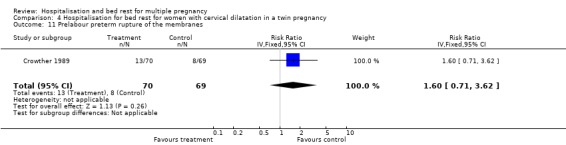
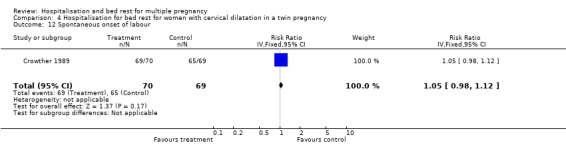
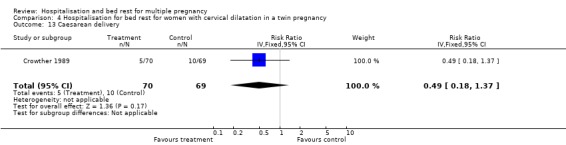
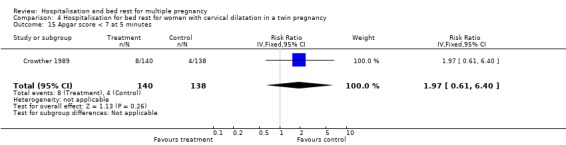
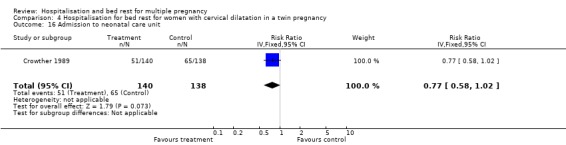
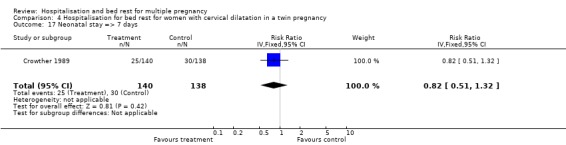
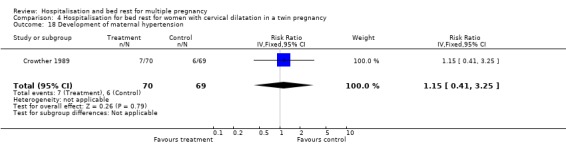
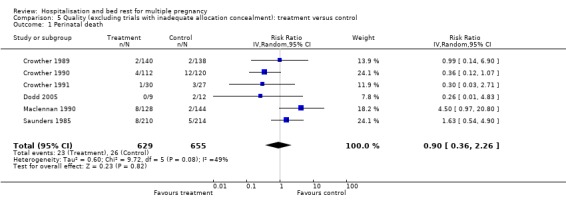
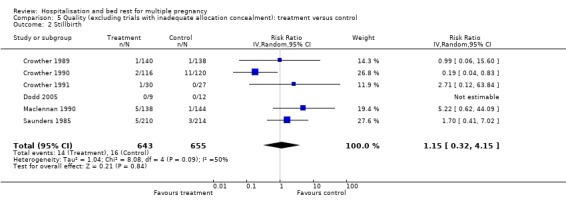
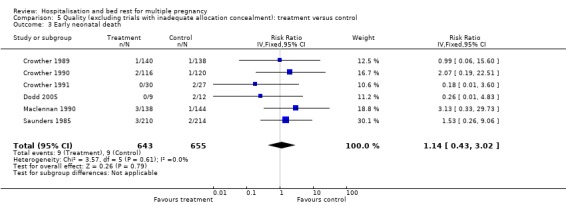
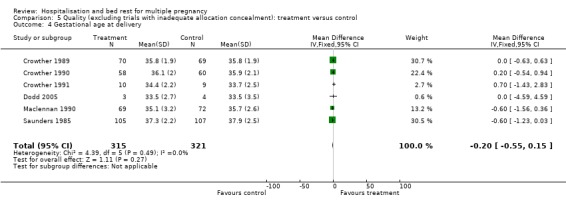
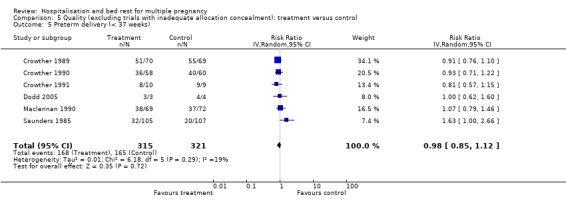
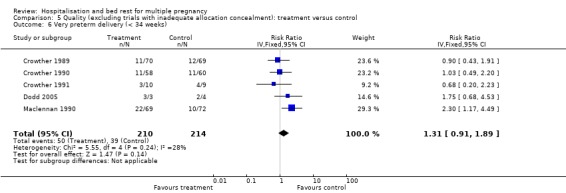
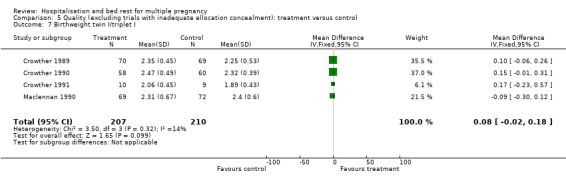
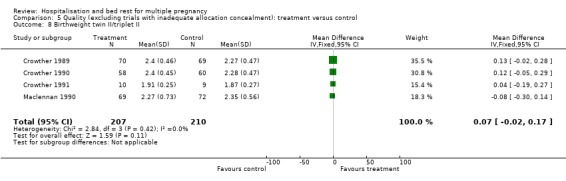
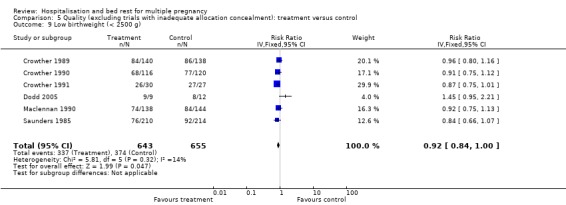
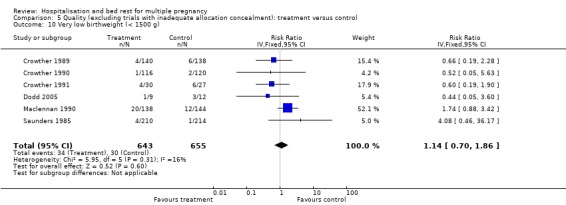
Main results: We included seven trials which involved 713 women and 1452 babies. Routine bed rest in hospital for multiple pregnancy did not reduce the risk of preterm birth, or perinatal mortality. There was substantial heterogeneity related to perinatal death and stillbirth unaccounted for by trial quality. There was a suggestion of a decreased number of low birthweight infants (less than 2500 g) born to women in the routinely hospitalised group (risk ratio (RR) 0.92; 95% confidence interval (CI) 0.85 to 1.00). No differences were seen in the number of very low birthweight infants (less than 1500 g). No support for the policy was found for other neonatal outcomes. No information is available on developmental outcomes for infants in any of the trials.For the secondary maternal outcomes reported of developing hypertension and caesarean delivery, no differences were seen. Women's views about the care they received were reported rarely.In the subgroup analyses for women with an uncomplicated twin pregnancy, with cervical dilation prior to labour with a twin pregnancy and with a triplet pregnancy, no differences were seen in any primary and secondary neonatal outcomes and maternal outcomes.
Authors' conclusions: There is currently not enough evidence to support a policy of routine hospitalisation for bed rest in multiple pregnancy. No reduction in the risk of preterm birth or perinatal death is evident, although there is a suggestion that fetal growth may be improved. For women with an uncomplicated twin pregnancy the results of this review show no benefit from routine hospitalisation for bed rest. Until further evidence is available, the policy cannot be recommended for routine clinical practice.
Conflict of interest statement
CA Crowther was chief investigator on four of the trials included in this review.
Figures


Update of
-
Hospitalisation and bed rest for multiple pregnancy.Cochrane Database Syst Rev. 2001;(1):CD000110. doi: 10.1002/14651858.CD000110. Cochrane Database Syst Rev. 2001. Update in: Cochrane Database Syst Rev. 2010 Jul 07;(7):CD000110. doi: 10.1002/14651858.CD000110.pub2. PMID: 11279677 Updated.
References
References to studies included in this review
Crowther 1989 {published data only}
-
- Crowther CA, Neilson JP, Verkuyl DAA, Bannerman C, Ashurst HM. Preterm labour in twin pregnancies: can it be prevented by hospital admission?. British Journal of Obstetrics and Gynaecology 1989;96:850‐3. - PubMed
Crowther 1990 {published data only}
-
- Crowther CA, Verkuyl DAA, Neilson JP, Bannerman C, Ashurst HM. The effects of hospitalization for rest on fetal growth, neonatal morbidity and length of gestation in twin pregnancy. British Journal of Obstetrics and Gynaecology 1990;97:872‐7. - PubMed
Crowther 1991 {published data only}
-
- Crowther CA, Verkuyl D, Ashworth M, Bannerman C, Ashurst H. The effects of hospitalisation for bed rest on duration of gestation, fetal growth and neonatal morbidity in triplet pregnancy. Acta Geneticae Medicae et Gemellologiae 1991;40:63‐8. - PubMed
Dodd 2005 {published data only}
Hartikainen‐Sorri 1984 {published and unpublished data}
-
- Hartikainen‐Sorri AL, Jouppila P. Is routine hospitalization needed in antenatal care of twin pregnancy?. Journal of Perinatal Medicine 1984;12:31‐4. - PubMed
Maclennan 1990 {published data only}
-
- MacLennan AH, Green RC, O'Shea R, Brookes C, Morris D. Routine hospital admission in twin pregnancy between 26 and 30 weeks' gestation. Lancet 1990;335:267‐9. - PubMed
Saunders 1985 {published data only}
-
- Saunders MC, Dick JS, Brown I McL, McPherson K, Chalmers I. The effects of hospital admission for bed rest on the duration of twin pregnancy: a randomised trial. Lancet 1985;2:793‐5. - PubMed
References to studies excluded from this review
Gummerus 1985 {published data only}
-
- Gummerus M, Halonen O. Prophylactic long‐term oral tocolysis of multiple pregnancies. British Journal of Obstetrics and Gynaecology 1987;94(3):249‐51. - PubMed
-
- Gummerus M, Halonen O. The merits of betamimetic treatment and bed rest in multiple pregnancies [Vuodelevon ja beetasympatomimeetthoidon vaikutus monisikioisessa raskaudessa]. Duodecim 1985;101:1966‐71. - PubMed
References to studies awaiting assessment
al‐Najashi 1996 {published data only}
-
- al‐Najashi SS, al‐Mulhim AA. Prolongation of pregnancy in multiple pregnancy. International Journal of Gynecology & Obstetrics 1996;54(2):131‐5. - PubMed
Younis 1990 {published data only}
-
- Younis JS, Sadovsky E, Eldar‐Geva T, Mildwidsky A, Zeevi D, Zajicek G. Twin gestations and prophylactic hospitalization. International Journal of Gynecology & Obstetrics 1990;32(4):325‐30. - PubMed
Additional references
Clarke 2000
-
- Clarke M, Oxman AD, editors. Cochrane Reviewers’ Handbook 4.1 [updated June 2000]. In: Review Manager (RevMan) [Computer program]. Version 4.1. Oxford, England: The Cochrane Collaboration, 2000.
Crowther 2005
-
- Crowther CA, Dodd JM. Multiple pregnancy. In: James D, Steer P, Weiner C, Gonik B editor(s). High risk pregnancy. 3rd Edition. Elsevier, 2005.
Deeks 2001
-
- Deeks JJ, Altman DG, Bradburn MJ. Statistical methods for examining heterogeneity and combining results from several studies in meta‐analysis. In: Egger M, Davey Smith G, Altman DG editor(s). Systematic reviews in health care: meta‐analysis in context. London: BMJ Books, 2001.
Higgins 2008
-
- Higgins JPT, Green S, editors. Cochrane Handbook for Systematic Reviews of Interventions Version 5.0.1 [updated September 2008]. The Cochrane Collaboration, 2008. Available from www.cochrane‐handbook.org.
Houlton 1982
-
- Houlton MCC, Marivate M, Philpott RHP. Factors associated with preterm labour and changes in the cervix before labour in twin pregnancy. British Journal of Obstetrics and Gynaecology 1982;89:190‐4. - PubMed
McKeown 1952
-
- McKeown T, Record R. Observation on fetal growth in multiple pregnancy in man. Journal of Endocrinology 1952;8:386‐401. - PubMed
Neilson 1988
-
- Neilson JP, Verkuyl DAA, Crowther CA, Bannerman C. Preterm labour in twin pregnancies: Prediction by cervical assessment. Obstetrics & Gynecology 1988;72:719‐23. - PubMed
RevMan 2008 [Computer program]
-
- The Cochrane Collaboration. Review Manager (RevMan). Version 5.0. Copenhagen, The Nordic Cochrane Centre: The Cochrane Collaboration, 2008.
Russell 1952
-
- Russell J. Maternal and fetal hazards associated with twin pregnancy. Journal of Obstetrics and Gynaecology of the British Commonwealth 1952;59:208‐13. - PubMed
References to other published versions of this review
Crowther 1991a
-
- Crowther CA. Hospitalisation for bed rest in multiple pregnancy. In: Chalmers I (ed) Oxford Database of Perinatal Trials. Version 1.2. Disk Issue 6, Autumn 1991.
Crowther 1991b
-
- Crowther CA. Hospitalisation for bed rest in twin pregnancy. In: Chalmers I (ed) Oxford Database of Perinatal Trials. Version 1.2. Disk Issue 6, Autumn 1991.
Crowther 1991c
-
- Crowther CA. Hospitalisation for bed rest in triplet pregnancy. In: Chalmers I (ed) Oxford Database of Perinatal Trials. Version 1.2. Disk Issue 6, Autumn 1991.
Crowther 1991d
-
- Crowther CA. Hospitalisation for cervical dilatation in twin pregnancy. In: Chalmers I (ed) Oxford Database of Perinatal Trials. Version 1.2. Disk Issue 6, Autumn 1991.
Crowther 1995a
-
- Crowther CA. Hospitalisation for bed rest in multiple pregnancy. [revised 05 October 1993]. In: Keirse MJNC, Renfrew MJ, Neilson JP, Crowther C (eds.) Pregnancy and Childbirth Module. In: The Cochrane Pregnancy and Childbirth Database [database on disk and CDROM]. The Cochrane Collaboration; Issue 2, Oxford: Update Software; 1995.
Crowther 1995b
-
- Crowther CA. Hospitalisation for bed rest in triplet pregnancy. [revised 05 October 1993]. In: Keirse MJNC, Renfrew MJ, Neilson JP, Crowther C (eds.) Pregnancy and Childbirth Module. In: The Cochrane Pregnancy and Childbirth Database [database on disk and CDROM]. The Cochrane Collaboration; Issue 2, Oxford: Update Software; 1995.
Crowther 1995c
-
- Crowther CA. Hospitalisation for bed rest in twin pregnancy. [revised 05 October 1993]. In: Keirse MJNC, Renfrew MJ, Neilson JP, Crowther C (eds.) Pregnancy and Childbirth Module. In: The Cochrane Pregnancy and Childbirth Database [database on disk and CDROM]. The Cochrane Collaboration; Issue 2, Oxford: Update Software; 1995.
Crowther 1995d
-
- Crowther CA. Hospitalisation for cervical dilation in twin pregnancy. [revised 05 October 1993]. In: Keirse MJNC, Renfrew MJ, Neilson JP, Crowther C (eds.) Pregnancy and Childbirth Module. In: The Cochrane Pregnancy and Childbirth Database [database on disk and CDROM]. The Cochrane Collaboration; Issue 2, Oxford: Update Software; 1995.
Crowther 1997
-
- Crowther CA. Hospitalisation for bedrest in multiple pregnancy. In: Neilson JP, Crowther CA, Hodnett ED, Hofmeyr GJ (eds.) Pregnancy and Childbirth Module of The Cochrane Database of Systematic Reviews [updated 01 September 1997]. Available in The Cochrane Library [database on disk and CDROM]. The Cochrane Collaboration; Issue 3. Oxford: Update Software; 1997. Updated quarterly.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources