

Circuit class therapy for improving mobility after stroke
- PMID: 20614460
- PMCID: PMC6464862
- DOI: 10.1002/14651858.CD007513.pub2
Circuit class therapy for improving mobility after stroke
Update in
-
Circuit class therapy for improving mobility after stroke.Cochrane Database Syst Rev. 2017 Jun 2;6(6):CD007513. doi: 10.1002/14651858.CD007513.pub3. Cochrane Database Syst Rev. 2017. PMID: 28573757 Free PMC article.
Abstract
Background: Circuit class therapy (CCT) offers a supervised group forum for people after stroke to practise tasks, enabling increased practise time without increasing staffing.
Objectives: To examine the effectiveness and safety of CCT on mobility in adults with stroke.
Search strategy: We searched the Cochrane Stroke Group Trials Register (last searched October 2009), the Cochrane Central Register of Controlled Trials (CENTRAL) (The Cochrane Library, Issue 2, 2009), MEDLINE (1950 to November 2008), EMBASE (1980 to November 2008), CINAHL (1982 to November 2008) and 14 other electronic databases (to November 2008). We also searched proceedings from relevant conferences, reference lists and unpublished theses; contacted authors of published trials and other experts in the field; and searched relevant clinical trials and research registers.
Selection criteria: Randomised or quasi-randomised controlled trials including people over 18 years old diagnosed with stroke of any severity, at any stage, or in any setting, receiving CCT.
Data collection and analysis: Two review authors independently selected trials for inclusion, assessed methodological quality and extracted data.
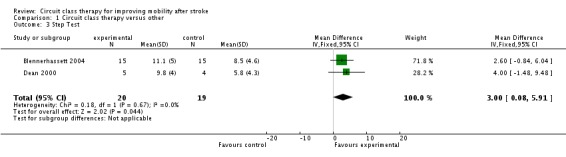
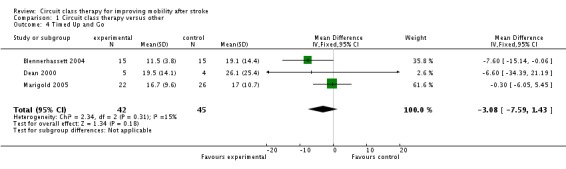
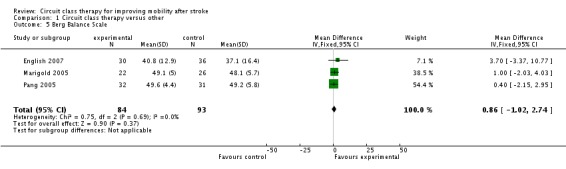
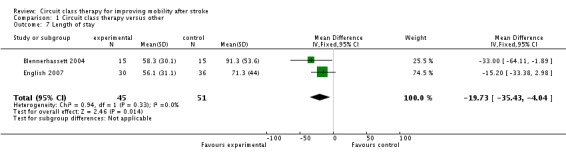
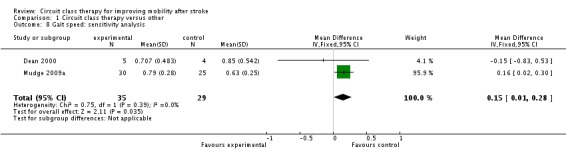
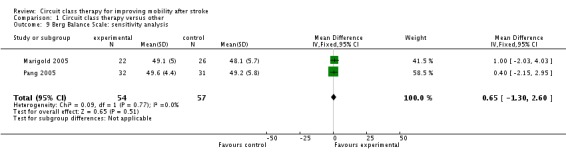
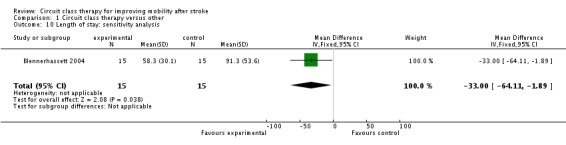
Main results: We included six trials involving 292 participants. Participants were long-term stroke survivors living in the community or receiving inpatient rehabilitation. All could walk 10 metres with or without assistance. Four studies measured walking capacity and three measured gait speed, demonstrating that CCT was superior to the comparison intervention (Six Minute Walk Test: mean difference (MD), fixed 76.57 metres, 95% confidence interval (CI) 38.44 to 114.70, P < 0.0001; gait speed: MD, fixed 0.12 m/s, 95% CI 0.00 to 0.24, P = 004). Two studies measured balance, showing a superior effect in favour of CCT (Step Test: MD, fixed 3.00 steps, 95% CI 0.08 to 5.91, P = 0.04; activities-specific balance and confidence: MD, fixed 7.76, 95% CI 0.66 to 14.87, P = 0.03). Studies also measured other balance items showing no difference in effect. Length of stay (two studies) showed a significant effect in favour of CCT (MD, fixed -19.73 days, 95% CI -35.43 to -4.04, P = 0.01). Only two studies measured adverse events (falls during therapy): all were minor.
Authors' conclusions: CCT is safe and effective in improving mobility for people after moderate stroke and may reduce inpatient length of stay. Further research is required, investigating quality of life, participation and cost-benefits, that compares CCT to standard care and that also investigates the differential effects of stroke severity, latency and age.
Conflict of interest statement
Both authors have published a trial investigating the use of CCT with people with stroke (English 2007).
Figures





References
References to studies included in this review
-
- Blennerhassett J, Dite W. Additional task‐related practice improves mobility and upper limb function early after stroke: a randomised controlled trial. Australian Journal of Physiotherapy 2004;50:219‐24. - PubMed
-
- Dean C, Richards C, Malouin F. Task‐related circuit training improves performance of locomotor tasks in chronic stroke: a randomised controlled pilot trial. Archives of Physical Medicine and Rehabilitation 2000;81:409‐17. - PubMed
-
- English C, Hillier S, Stiller K, Warden‐Flood A. Circuit class therapy versus individual physiotherapy sessions during inpatient stroke rehabilitation: a controlled trial. Archives of Physical Medicine and Rehabilitation 2007;88:955‐63. - PubMed
-
- Mudge S, Stott N, Barber P. Circuit‐based rehabilitation improves gait endurance but not usual walking activity in chronic stroke: a randomised clinical trial. Archives of Physical Medicine and Rehabilitation 2009;90(12):1989‐96. - PubMed
References to studies excluded from this review
-
- Blennerhassett J. The value of circuit classes in stroke rehabilitation. International Journal of Therapy and Rehabilitation 2008;15(6):272.
-
- Brogårdh C, Sjölund B. Constraint‐induced movement therapy in patients with stroke: a pilot study on effects of small group training and of extended mitt use. Clinical Rehabilitation 2006;20:218‐27. - PubMed
-
- English C, Hillier S, Stiller K. Incidence and severity of shoulder pain does not increase with the use of circuit class therapy during inpatient stroke rehabilitation: a controlled trial. Australian Journal of Physiotherapy 2008;54:41‐6. - PubMed
-
- French B, Leathley M, Sutton C, McAdam J, Thomas A, Forster A, et al. A systematic review of repetitive functional task practice with modelling of resource use, costs and effectiveness. Health Technology Assessment 2008;12(30):1‐117. - PubMed
Additional references
-
- Begg S, Vos T, Barker B, Stevenson C, Stanley L, Lopez AD. The burden of disease and injury in Australia 2003. Australian Institute of Health and Welfare. Canberra2007.
-
- Bernhardt J, Dewey H, Thrift A, Donnan G. Inactive and alone. Physical activity within the first 14 days of acute stroke unit care. Stroke 2004;35:1005‐9. - PubMed
-
- Cox KL, Burke V, Gorley TJ, Beilin LJ, Puddy IB. Controlled comparison of retention and adherence in home‐ vs center‐initiated exercise interventions in women ages 40‐65 years: the SWEAT study (Sedentary Women Exercise Adherence Trial). Preventive Medicine 2003;36:17‐29. - PubMed
-
- Dean C, Richards C, Malouin F. Walking speed over 10 metres overestimates locomotor capacity after stroke. Clinical Rehabilitation 2001;15:415‐21. - PubMed
-
- Dewey H, Sturm J, Donnan G, Macdonell R, McNeil J, Thrift A. Incidence and outcome of subtypes of ischaemic stroke: initial results from the North East Melbourne Stroke Incidence Study (NEMESIS). Cerebrovascular Diseases 2003;15:133‐9. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical