

Impact of race on hyperparathyroidism, mineral disarrays, administered vitamin D mimetic, and survival in hemodialysis patients
- PMID: 20614473
- PMCID: PMC3179282
- DOI: 10.1002/jbmr.177
Impact of race on hyperparathyroidism, mineral disarrays, administered vitamin D mimetic, and survival in hemodialysis patients
Erratum in
- J Bone Miner Res. 2011 Feb;26(2):439
Abstract
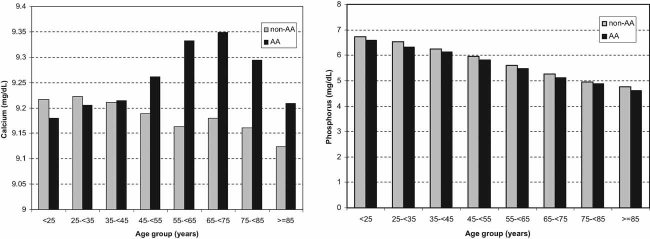
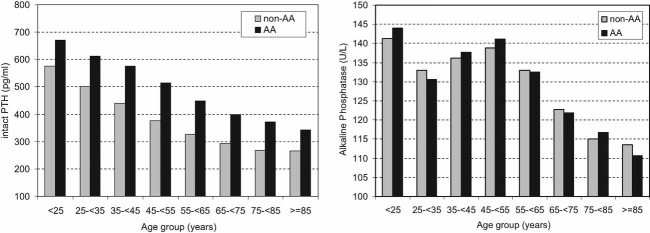
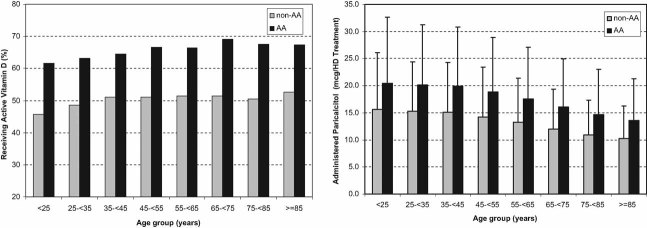
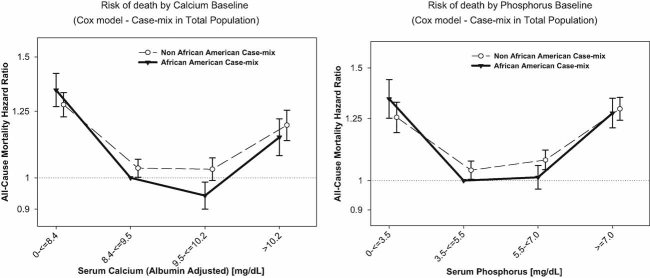
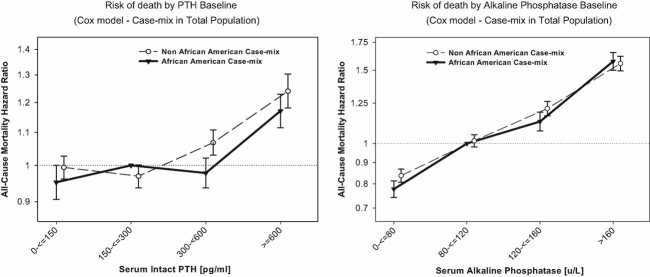
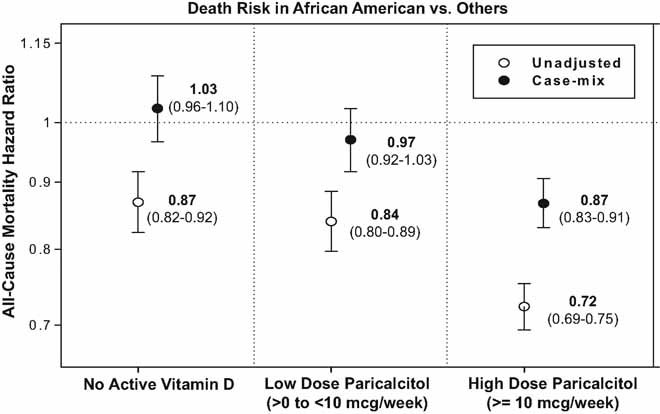
Blacks have high rates of chronic kidney disease, are overrepresented among the US dialysis patients, have higher parathyroid hormone levels, but greater survival compared to nonblacks. We hypothesized that mineral and bone disorders (MBDs) have a bearing on survival advantages of black hemodialysis patients. In 139,328 thrice-weekly treated hemodialysis patients, including 32% blacks, in a large dialysis organization, where most laboratory values were measured monthly for up to 60 months (July 2001 to June 2006), we examined differences across races in measures of MBDs and survival predictabilities of these markers and administered the active vitamin D medication paricalcitol. Across each age increment, blacks had higher serum calcium and parathyroid hormone (PTH) levels and almost the same serum phosphorus and alkaline phosphatase levels and were more likely to receive injectable active vitamin D in the dialysis clinic, mostly paricalcitol, at higher doses than nonblacks. Racial differences existed in mortality predictabilities of different ranges of serum calcium, phosphorus, and PTH but not alkaline phosphatase. Blacks who received the highest dose of paricalcitol (>10 µg/week) had a demonstrable survival advantage over nonblacks (case-mix-adjusted death hazard ratio = 0.87, 95% confidence level 0.83-0.91) compared with those who received lower doses (<10 µg/week) or no active vitamin D. Hence, in black hemodialysis patients, hyperparathyroidism and hypercalcemia are more prevalent than in nonblacks, whereas hyperphosphatemia or hyperphosphatasemia are not. Survival advantages of blacks appear restricted to those receiving higher doses of active vitamin D. Examining the effect of MBD modulation on racial survival disparities of hemodialysis patients is warranted.
Copyright © 2010 American Society for Bone and Mineral Research.
Figures
References
-
- Norris KC, Agodoa LY. Unraveling the racial disparities associated with kidney disease. Kidney Int. 2005;68:914–924. - PubMed
-
- Agodoa L. Racial disparities in kidney health: the puzzle to solve. Am J Kidney Dis. 2002;40:1337–1339. - PubMed
-
- Agodoa L, Eggers P. Racial and ethnic disparities in end-stage kidney failure: survival paradoxes in African-Americans. Semin Dial. 2007;20:577–585. - PubMed
-
- United States Renal Data System. United States Renal Data System 2006 annual data report: atlas of chronic kidney disease and end-stage renal disease in the United States. Am J Kidney Dis. 2007;49:S1–296. - PubMed
-
- United States Renal Data System. Excerpts from the USRDS 2005 annual data report: atlas of end-stage renal disease in the United States, National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases. Am J Kid Dis. 2006;471:1–286.
